Blood Pressure, Body Mass Index and Risk of End-Stage Renal Disease among Men and Women in China
Blood Pressure, Body Mass Index and Risk of End-Stage Renal Disease among Men and Women in China
Outline
The association between blood pressure (BP), body mass index (BMI) and risk of end-stage renal disease (ESRD) has not been well characterized in Asian populations. We examined the relationship between BP, BMI and risk of ESRD in a prospective cohort study of 169,871 Chinese men and women aged 40 years and older. Data on BP, body weight, height and covariables were obtained at a baseline examination in 1991 using a standard protocol. BMI was calculated as weight in kilograms divided by the square of height in meters (kg/m2). Follow-up evaluation was conducted in 1999-2000, with a response rate of 93.4%. During 1,236,422 person-years of follow-up, 380 participants (30.7 cases per 100,000 person-years) initiated renal replacement therapy or died from renal failure. A strong, graded, and significant relationship between BP and incidence of all-cause and glomerulonephritis-related ESRD was present, independent of important covariables. Compared to those with normal BP, relative risks (95% confidence interval) of all-cause ESRD for prehypertension, and stage-1 and stage-2 hypertension were 1.30 (0.98-1.74), 1.47 (1.06-2.06), and 2.60 (1.89-3.57), respectively P<0.001 for trend). The corresponding relative risks (95% confidence interval) of glomerulonephritis-related ESRD were 1.32 (0.82-2.11), 1.48 (0.83-2.61), and 3.40 (2.02-5.74), respectively P<0.001 for trend). Systolic BP was a stronger predictor of ESRD than diastolic BP or pulse pressure. After adjustment for age, sex, geographic region (north vs. south China), urbanization (urban vs. rural residence), education, physical activity, cigarette smoking, and alcohol consumption, a J-shaped association between BMI and all-cause ESRD was observed. Compared to those with normal body weight (BMI 18.5-24.9 kg/m2), the multivariate adjusted relative risks (95% confidence interval) of all-cause ESRD for underweight (BMI <18.5 kg/m2), overweight (BMI 25.0-29.9 kg/m2), and obesity (BMI ≥30 kg/m2) were 1.39 (1.02-1.91), 1.21 (0.92-1.59), and 2.14 (1.39-3.29), respectively. The J-shaped association existed even after additional adjustment for baseline systolic blood pressure and history of diabetes and cardiovascular disease.
The current study provides important novel information on the association between BP and glomerulonephritis-related ESRD, the leading assigned cause of ESRD in China. This study also documents the importance of high BP as a modifiable risk factor for ESRD. The results from this large cohort indicate that Chinese adults who are underweight, overweight, or obese have a higher rate of ESRD. Strategies aimed at prevention of ESRD in China need to incorporate the prevention, treatment, and control of high BP and to maintain an optimal body weight.
End-stage renal disease (ESRD) is both a personal tragedy and a significant public health problem worldwide. Patients with ESRD suffer a poor quality of life and have a shorter life expectancy compared to individuals of the same age in the general population [1,2]. Therefore, identifying modifiable risk factors for ESRD will help to develop strategies for prevention in the population.
Hypertension is well recognized as an independent risk factor for developing kidney disease (3, 4). However, few prospective cohort studies have examined the relationship between a broad range of the blood pressure (BP) distribution and the risk of ESRD (5,6,7 and 8). The relative importance of systolic or diastolic BP or pulse pressure on the risk of ESRD remains to be resolved. Additionally, the role of elevated BP and the development of non-hypertensive ESRD, especially glomerulonephritis-related ESRD, has not been well established. Furthermore, limited information exists on the relationship between BP and ESRD in Chinese populations, where glomerulonephritis is the most commonly assigned cause of renal failure (9,10). Understanding the modifiable risk factors of ESRD is critically important for the development and implementation of prevention strategies.
Overweight and obesity are important risk factors for cardiovascular disease and premature death [30]. Obesity is also an important modifiable risk factor for hypertension and diabetes, both of which are strong predictors for the development and progression of kidney disease [31,32 and 33]. However, the relationship between excess weight and risk of ESRD remains unclear. A J-shaped association between body mass index (BMI) and proteinuria has been reported in one study [34], while other studies have reported a direct association [35,36,37,38,39 and 40] or an inverse association [41] between BMI and development of ESRD. Furthermore, previous studies have been mainly conducted among Western populations, which have different epidemiologic features of renal disease than in China where the most common underlying assigned cause for ESRD is glomerulonephritis [42].
The purposes of the current study are three-fold: to determine the incidence and relative risk of ESRD across a wide range of BP levels; to compare the relative importance of systolic, diastolic, or pulse pressure on predicting the incidence of ESRD; to examine the consistency of the associations between BP and subtype of ESRD; and to examine the relationship between BMI and development of all-cause ESRD in a large, prospective cohort study of a national sample of men and women aged 40 years and older in China.
1. METHODS
1.1 Study Population
In the 1991 China National Hypertension Survey, a multistage random cluster sampling design was used to select a representative sample of the general Chinese population (11). A total of 950,356 men and women aged 15 years and older were selected from all 30 provinces. In 1999, investigators from each province were invited to participate in the China National Hypertension Survey Epidemiology Follow-up Study (CHEFS). Of the 30 provinces included in the 1991 study, 13 provinces were not included in the follow-up study because participants’ contact information was not available. However, sampling for the 1991 survey was conducted independently within each province and study participants included in the follow-up study were evenly distributed among the different geographic regions of the entire country representing various stages of economic development. Overall, 169,871 (83,533 men and 86,338 women) who were 40 years or older at the baseline examination were eligible for the follow-up study. From this population, a total of 158,666 participants or their proxies (93.4%) were identified and interviewed as part of the follow-up study. After excluding those with ESRD at baseline (n=34), those with missing BP measures (n=267) or those with missing body weight or height values(n=14,830), data from 158,365 or 143,802 participants were included in the BP or BMI analysis, respectively.
1.2 Baseline Examination
Baseline data collection occurred during a single clinic visit conducted at a local field center. Data on demographic characteristics, medical history, and lifestyle risk factors were obtained using a standard questionnaire administered by trained staff. Physical activity was based on work-related activities because leisure-time physical activity was uncommon. Cigarette smoking was defined as smoking at least one cigarette per day for one or more years. Data were collected on the amount and type of alcohol consumed during the previous year.
1.3 Baseline Examination
Three BP measurements were obtained from participants by trained nurses or doctors according to a standard protocol adapted from procedures recommended by the American Heart Association (14). BP was measured on the right arm in the sitting position using a standardized mercury sphygmomanometer after the participant had been resting quietly for at least 5 minutes. In addition, participants were advised to avoid exercising, cigarette smoking, and consuming alcohol, coffee or tea for at least 30 minutes before their BP measurement. The first and fifth Korotkoff sounds were recorded as systolic and diastolic BP, respectively (11).
Body weight and height were measured once during the visit by trained observers using a standard protocol and with the participant wearing light indoor clothing and without shoes. Height was measured with the participant standing on a firm, level surface at a right angle to the vertical board of the height measurement device. A height board mounted at a 90° angle to a calibrated vertical height bar was used. BMI was calculated as weight in kilograms divided by height in meters squared (kg/m2). Following internationally recognized definitions [44,45], underweight was defined as a BMI <18.5 kg/m2, normal weight as a BMI of 18.5 to 24.9 kg/m2, overweight as a BMI of 25.0 to 29.9 kg/m2, and obesity as a BMI ≥30 kg/m2.
1.4 Follow-up Data Collection
Follow-up examinations were conducted in 1999 and 2000 and included tracking study participants or their proxies to a current address; performing in-depth interviews to ascertain disease status and vital information; and obtaining hospital records and death certificates. Interviewed persons were asked whether the participant received treatment for ESRD since 1991. Additionally, death certificates were obtained for all deceased participants. All ESRD events reported during the in-person interview were verified by obtaining medical records or death certificates from the local hospital, public health department, or police department. ESRD was defined as renal replacement therapy (renal transplantation or dialysis) or death from renal failure. Trained study staff visited all hospitals and dialysis units where patients received their treatment. The participants’ hospital records, including medical history, physical examination findings, laboratory test results, discharge diagnosis and/or autopsy findings were abstracted by study staff using a standard form. Treatment information, such as hemodialysis, peritoneal dialysis, and kidney transplantation was also collected. In addition, photocopies of selected sections of the participant’s inpatient record, discharge summary, and pathology reports were obtained.
An endpoint assessment committee in each province reviewed and confirmed (or rejected) the hospital’s discharge diagnosis and cause of death based on the abstracted information using prespecified criteria. A study-wide endpoint assessment committee at the Chinese Academy of Medical Sciences in Beijing independently reviewed all ESRD cases. Each ESRD case was verified by two committee members, the results were compared, and discrepancies were adjudicated by discussion involving additional committee members. Deaths were classified as being due to renal failure if one of the following ICD-9-CM codes was given on the death certificate as the underlying cause: 403-404 (hypertensive renal disease), 250.4 (diabetes mellitus with nephropathy), 274.1 (gouty nephropathy), 275.4 (nephrocalcinosis), 593.3, 593.4, 593.5, 593.7, 593.8, 593.9 (other kidney disorders), 596 (bladder-neck obstruction), 600 (hyperplasia of prostate), 753.1 (cystic kidney disease), 580-589 (nephritis, nephritic syndrome, or nephrosis), 590 (infection of the kidney), 591 (hyrdonephrosis), and 592 (calculus of the kidney and ureter) (15).
This study was approved by the Tulane University Health Sciences Center Institutional Review Board and the Cardiovascular Institute and Fu Wai Hospital Ethics Committee. Written informed consent was obtained from all study participants at their follow-up visit.
1.5 Statistical Analysis
Study participants were grouped according to the JNC-7 classification of BP as measured at the baseline examination (normal BP, systolic BP <120 mm Hg and diastolic BP <80 mm Hg; prehypertension, systolic BP of 120-139 mm Hg or diastolic BP of 80-89 mm Hg; stage 1 hypertension, systolic BP 140-159 mm Hg or diastolic BP 90-99 mm Hg; and stage 2 hypertension, systolic BP ≥160 mm Hg or diastolic BP ≥ 100 mm Hg) (16). Participants who reported current use of antihypertensive medication were included in the stage 2 hypertension category. Additionally, systolic, diastolic, and pulse pressures were categorized separately by quintiles (systolic BP: <108.5, 108.5-118.5, 118.5-128.5, 128.5-141, and ≥ 141; diastolic BP: <68, 68-74, 74-80, 80-87, and ≥87; and pulse pressure <37, 37-42.5, 42.5-50, 50-60, and ≥60). Study participants were grouped according to BMI category (underweight, normal weight, overweight, and obesity) and age-standardized incidence rates were calculated for each category using the age distribution of the Chinese population from year 2000 census data as the standard.
Person-years of follow-up were calculated from the date of the baseline examination until the date of death, development of ESRD, or the follow-up interview, whichever occurred first, for each study participant and grouped according to sex and to age in 5-year categories. Cumulative incidence of ESRD was calculated by JNC-7 BP category using the Kaplan-Meier method and compared across categories using the log-rank test (17,18). Age-standardized incidence rates were calculated using the 5-year age-specific incidence and the age distribution of the Chinese population from year 2000 census data.
Cox proportional hazards models were used to examine the multivariate adjusted relationships of systolic, diastolic and pulse pressure with the incidence of ESRD. Initial models included adjustment for age and sex. Subsequent models included additional adjustment for geographic region (north vs. south China), urbanization (urban vs. rural residence), education(high school or greater), BMI, physical activity, current cigarette smoking, alcohol drinking, and history of diabetes and cardiovascular disease (stroke or coronary heart disease). History of diabetes and cardiovascular disease were modeled as time-dependent variables in extended Cox models (19). Multivariate adjusted relative risks were calculated using study participants with normal BP as the reference group. These analyses were conducted separately for all-cause ESRD, glomerulonephritis-related ESRD, non-glomerulonephritis-related ESRD, and unknown cause of ESRD. Population attributable risks were calculated for each BP category. Additionally, adjusted relative risks for each quintile of systolic, diastolic, and pulse pressure as well as adjusted relatives risks associated with one standard deviation higher BP were used to compare the predictive significance of systolic, diastolic, and pulse pressures. Analyses were also performed with both systolic and diastolic BP in the models (or equivalently, both pulse pressure and systolic BP or pulse pressure and diastolic BP) simultaneously.
Relative risks were calculated using normal weight (BMI 18.5-24.9 kg/m2) as the reference group. The presence of a linear trend was tested using the medians of each BMI group treated as a continuous variable. The presence of a non-linear association was tested using quadratic terms. The main multivariate analysis did not include adjustment for history of diabetes and cardiovascular disease (stroke or coronary heart disease), or systolic blood pressure since these factors are likely intermediate variables in the causal pathway between BMI and ESRD. However, these risk factors were included in additional analyses to examine the independent effect of BMI on the development of ESRD. History of diabetes and cardiovascular disease were modeled as time-dependent variables in extended Cox models [19].
Additionally, analyses were conducted stratified by sex and assigned underlying cause of ESRD (glomerulonephritis-related ESRD and non-glomerulonephritis-related ESRD). Methods that account for the multistage sample clustering were used to estimate variance in the Cox proportional hazards models [21]. Statistical analyses were conducted using SAS statistical software (version 9.1; SAS Institute Inc, Cary, NC).
2. RESULTS
During an average follow-up of 8.3 years (1,236,422 million person years of observation), 380 participants (30.7 cases per 100,000 person-years) initiated renal replacement therapy (n=121) or died from renal failure (n=259). Glomerulonephritis was the most common underlying assigned cause of ESRD (10.8 cases per 100,000 person years) followed by diabetes (5.0 cases per 100,000 person-years) and hypertension (2.7 cases per 100,000 person-years) (Table 19.1 ).
Baseline characteristics of the study participants are presented according to JNC-7 BP category in Table 19.2. Participants with higher BP were older, more likely to be male, living in northern China and urban areas, have a high school education, be current smokers, drink alcohol, physically inactive, overweight, and have a history of stroke or coronary heart disease.
Table 19.1 Crude Rates of End-Stage Renal Disease in 158,365 CHEFS Participants, China 1991-2000
Incidence
Mortality
No. Cases
Rate per 100,000 Person-Years
No. Cases
Rate per 100,000 Person-Years
Glomerulonephritis
133
10.8
95
7.7
Diabetic nephropathy
62
5.0
28
2.3
Hypertensive nephrosclerosis
33
2.7
19
1.5
Obstructive nephropathy
22
1.8
16
1.3
Other
15
1.2
6
0.5
Unknown
115
9.3
95
7.7
All-Cause
380
30.7
259
20.9
Table 19.2 Baseline Characteristics According to JNC-7 Blood Pressure Category in 158,365 CHEFS Participants, China 1991-2000
Blood pressure was categorized according to JNC VII guidelines: normal: systolic <120 mm Hg and diastolic <80 mm Hg; prehypertension: systolic 120-139 mm Hg or diastolic 80-89 mm Hg; stage 1 hypertension: systolic 140-159 mm Hg or diastolic 90-99 mm Hg; stage 2 hypertension: systolic ≥160 mm Hg or diastolic ≥100 mm Hg or use of anti-hypertensive medications.
* All data are mean (SD) or proportion. BP = blood pressure; CHD = coronary heart disease.
† Physical activity was assessed based on participants’ work-related activity only.
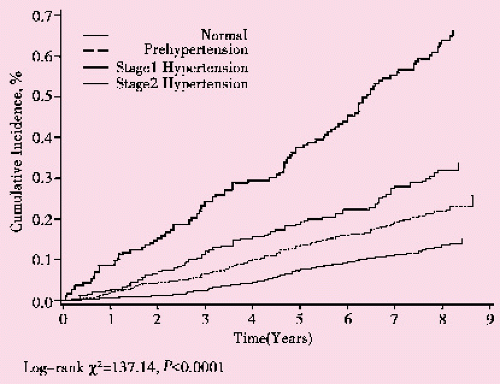
Figure 19.1 presents the cumulative incidence of all-cause ESRD during follow-up according to JNC-7 BP category. The cumulative incidence of all-cause ESRD after 8 years of follow-up was 0.14%, 0.23%, 0.34%, and 0.64% among participants with normal BP, pre-hypertension, stage-1 hypertension, and stage-2 hypertension, respectively (p for trend <0.001).
Figure 19.1 Cumulative incidence of all-cause end-stage renal disease according to JNC-7 blood pressure category among 158,365 CHEFS participants, China 1991-2000
The age-adjusted incidence and relative risk of all-cause ESRD and cause-specific ESRD by JNC-7 BP category are shown in Table 19.3. The risk of all-cause ESRD associated with higher BP was positive and graded after age, age-sex and multivariate adjustment. This graded and positive association between BP and all-cause ESRD, was consistent with glomerulonephritis-related ESRD, non-glomerulonephritis-related ESRD, and ESRD due to unknown causes. Population attributable risk estimates indicated that a large proportion of the ESRD cases were due to stage-2 hypertension. The positive and graded association between BP and risk of all-cause ESRD persisted when data were stratified by gender; however, the association was weaker in men than in women (Figure 19.2). Compared with participants with a normal BP, the multivariate adjusted relative risk (95% CI) of developing ESRD associated with prehypertension, stage-1, and stage-2 hypertension was 1.31 (.90-1.91), 1.09 (0.68-1.76), and 2.19 (1.41-3.40), respectively for men and 1.36 (0.86-2.14), 2.21 (1.36-3.58), and 3.43 (2.15-5.48), respectively for women.
Incidence and relative risk of all-cause ESRD by quintiles of systolic BP, diastolic BP, and pulse pressure are presented in Table 19.4. Incidence rates increased successively from lowest to highest quintile for each BP component. The relative risk of ESRD associated with higher systolic BP, diastolic BP, and pulse pressure was positive and graded after age-sex and multivariate adjustment. The multivariate adjusted relative risk associated with a higher BP was greatest for systolic BP and lowest for diastolic BP.
The multivariate adjusted relative risk of all-cause ESRD associated with each standard deviation BP (22.4 mm Hg, systolic BP; 12.1 mm Hg, diastolic BP; 16.1 mm Hg, pulse pressure) was higher for systolic BP and similar for diastolic BP and pulse pressure (Table 19.5 ). The strong and significant relationship between systolic BP and all-cause ESRD was not substantially changed in multivariate models that included diastolic BP and pulse pressure, separately. However, the relative risk of all-cause ESRD associated with diastolic BP and pulse pressure were reduced and no longer statistically significant after adjustment for systolic BP.
The mean BMI in the study population was 22.6 kg/m2 and 11.7% were underweight (BMI <18.5 kg/m2), 64.8% were normal weight (BMI 18.5-24.9 kg/m2), 20.3% were overweight (BMI 25-29.9 kg/m2), and 3.2% were obese (BMI ≥30 kg/m2) (Table 19.6 ). The proportion of men and women living in northern China and urban areas was higher in progressively higher BMI categories. The proportion of current cigarette smokers decreased at higher BMI among men. Among both men and women, the proportion of alcohol drinkers and heavy physical activity decreased with increasing BMI. Mean systolic and diastolic blood pressures increased with increasing BMI among both men and women. The proportion of participants with hypertension, a history of stroke and coronary heart disease increased with increasing BMI among men and women.
Table 19.3 Incidence Rates and Relative Risk of End-Stage Renal Disease by JNC-7 Blood Pressure Category in 158,365 CHEFS Participants, China 1991-2000
N/A = not applicable; population attributable risks were calculated for significant associations.
* Blood pressure was categorized according to JNC VII guidelines: normal: systolic <120 mm Hg and diastolic <80 mm Hg; prehypertension: systolic 120-139 mm Hg or diastolic 80-89 mm Hg; stage 1 hypertension: systolic 140-159 mm Hg or diastolic 90-99 mm Hg; stage 2 hypertension: systolic ≥160 mm Hg or diastolic ≥100 mm Hg or use of anti-hypertensive medications.
† Rates were standardized according to the 2000 census data for China’s population.
‡ Relative risks, with normal blood pressure as the reference category, were calculated using a Cox proportional hazards model adjusted for baseline age, gender, geographic region (north vs. south), urbanization (urban vs. rural), education, body mass index, physical activity, current cigarette smoking, alcohol drinking, and history of diabetes and cardiovascular disease, and stratified by sampling clusters.
Only gold members can continue reading. Log In or Register to continue
Aug 1, 2016 | Posted by drzezo in INFECTIOUS DISEASE | Comments Off on Blood Pressure, Body Mass Index and Risk of End-Stage Renal Disease among Men and Women in China
 Explore Route of Transmission for Kala-azar
Explore Route of Transmission for Kala-azar
 A Series of Etiological Epidemiology Studies on Kaschin-Beck Disease (1965-1993)
A Series of Etiological Epidemiology Studies on Kaschin-Beck Disease (1965-1993)
 Control and study of the first-time outbreak of angiostrongyliasis cantonensis in P.R. China
Control and study of the first-time outbreak of angiostrongyliasis cantonensis in P.R. China
 Discovery and Control of the HIV/AIDS Epidemic among Plasma Donors in China
Discovery and Control of the HIV/AIDS Epidemic among Plasma Donors in China



