Biopsy of Musculoskeletal Tumors
Jacob Bickels
Yair Gortzak
Martin M. Malawer
BACKGROUND
Biopsy is a fundamental step in the diagnosis of a musculoskeletal tumor. It should be regarded as the final diagnostic procedure, not as a mere shortcut to diagnosis.
Biopsy should be preceded by careful clinical evaluation and analysis of the imaging studies.2,6,10,11 Diagnosis of a musculoskeletal lesion is based on this triad of clinical, pathologic, and imaging findings, and all three must coincide or else the diagnosis should be questioned.2,6
Most biopsies are technically simple to perform. Decisions regarding the indication for biopsy, the specific region of the lesion for biopsy, and the anatomic approach and biopsy technique, however, can make the difference between a successful biopsy and a catastrophe.
A poorly performed biopsy could become an obstacle to proper diagnosis and may impede the performance of adequate and safe tumor resection.
BIOLOGIC BEHAVIOR OF MUSCULOSKELETAL TUMORS
Tumors arising in bone and soft tissues share characteristic patterns of biologic behavior, stemming from their common mesenchymal origin and anatomic environment. Those unique patterns form the basis of the staging system and current treatment strategies.
Histologically, sarcomas are categorized as being low, intermediate, or high grade based on tumor morphology, extent of pleomorphism, atypia, mitosis, and necrosis. Grading represents their biologic aggressiveness and correlates with the likelihood of metastases.
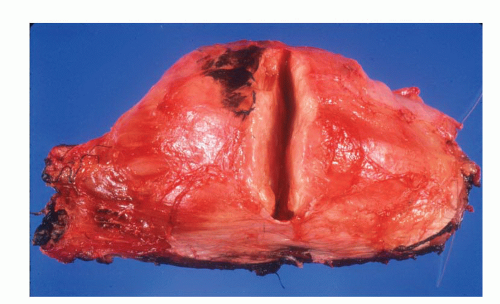
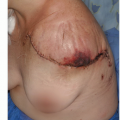
FIG 1 • A cut through a high-grade soft tissue sarcoma showing its thin pseudocapsule composed of compressed tumor cells and a fibrovascular zone of reactive inflammatory response.
Sarcomas form a solid mass that grows centrifugally with the periphery of the lesion being the least mature part. Unlike the true capsule that surrounds benign lesions, which is composed of compressed normal cells, sarcomas are generally enclosed by a reactive zone or pseudocapsule. This consists of compressed tumor cells and a fibrovascular zone of reactive tissue with a variable inflammatory component that interacts with the surrounding normal tissues (FIG 1).
In addition, these cells may break through the pseudocapsule to form metastases (“skip metastases”) within the same anatomic compartment in which the lesion is located. By definition, these are locoregional micrometastases that have not passed through the circulation (FIGS 2,3 and 4). This phenomenon
may be responsible for local recurrences that develop in spite of apparently negative margins after a resection. Although low-grade sarcomas regularly interdigitate into the reactive zone, they rarely form tumor skip nodules beyond that area.
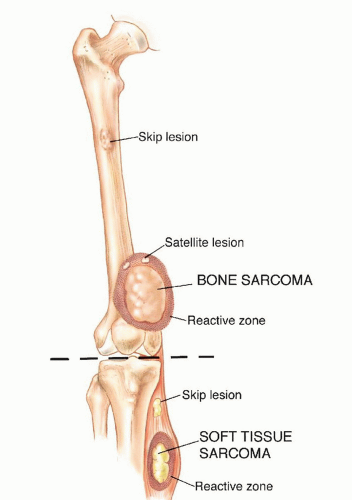
FIG 2 • Growth pattern of bone and soft tissue sarcomas. Sarcomas grow in a centripetal fashion, with the most immature part of the lesion at the growing edge. A reactive zone is formed between the tumor and the compressed surrounding normal tissues and may be invaded by tumor nodules that represent microextensions of the tumor (satellites) and not a metastatic phenomenon. High-grade sarcomas may present with tumor nodules that grow outside the reactive zone (skip lesions) but within the same anatomic compartment in which the lesion is located. This finding is documented preoperatively in less than 5% of patients. (Reprinted from Bickels J, Jelinek JS, Shmookler BM, et al. Biopsy of musculoskeletal tumors: current concepts. Clin Orthop Relat Res 1999;368:212-219.)
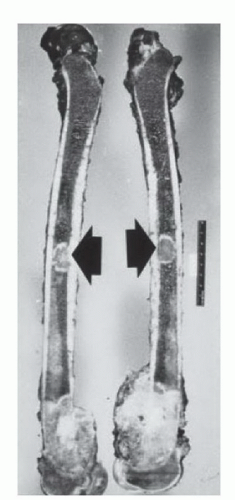
FIG 3 • High-grade sarcomas may break through the pseudocapsule to form skip metastases within the same anatomic compartment. Skip metastases (arrows) from an osteosarcoma of the distal femur.
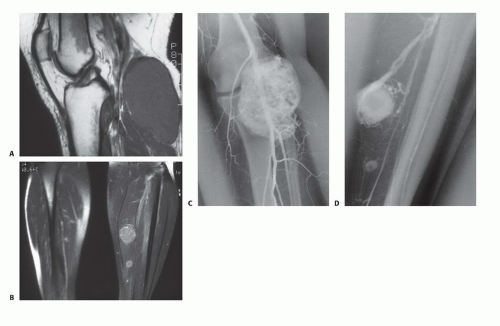
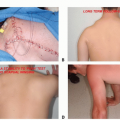
FIG 4 • A 40-year-old female who presented with a rapidly enlarging mass that had developed in her calf. Physical examination revealed a deep-seated, firm mass, 10 cm in diameter, located at the proximal aspect of the calf. MRI demonstrated the primary lesion (A) as well as additional two skip metastases in the substance of the soleus muscle (B). C,D. Angiogram of the lower extremity clearly shows all three lesions. (Reprinted from Bickels J, Jelinek JS, Shmookler BM, et al. Biopsy of musculoskeletal tumors: current concepts. Clin Orthop Relat Res 1999;368:212-219.)
Sarcomas respect anatomic borders. Local anatomy influences tumor growth by setting natural barriers to extension of the lesion. In general, sarcomas take the path of least resistance and initially grow within the anatomic compartment in which they arose. In a later stage, the walls of that compartment (either the cortex of a bone or aponeurosis of a muscle) are violated, and the tumor breaks into a surrounding compartment (FIGS 5 and 6).
Most bone sarcomas are bicompartmental at the time of presentation; they destroy the overlying cortex and extend directly into the adjacent soft tissues (FIG 7).
Soft tissue sarcomas may arise between compartments (extracompartmental) or in an anatomic site that is not walled off by anatomic barriers such as the intermuscular or subcutaneous planes. In the latter case, they remain extracompartmental and only at a later stage do they break into the adjacent compartment (FIG 8). Carcinomas, on the other hand, directly invade the surrounding tissues, irrespective of compartmental borders (FIG 9).
Unlike carcinomas, bone and soft tissue sarcomas disseminate almost exclusively through the blood. Hematogenous spread of extremity sarcomas is manifested by pulmonary involvement in the early stages and by bony involvement in later stages (FIG 10).
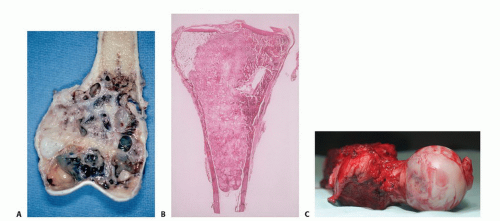 FIG 5 • High-grade osteosarcomas of the distal femur (A), proximal tibia (B), and proximal femur (C) showing tumor extension to the articular cartilage, which remains intact. This phenomenon allows intra-articular resection in most cases of juxtaarticular sarcomas of bone. |
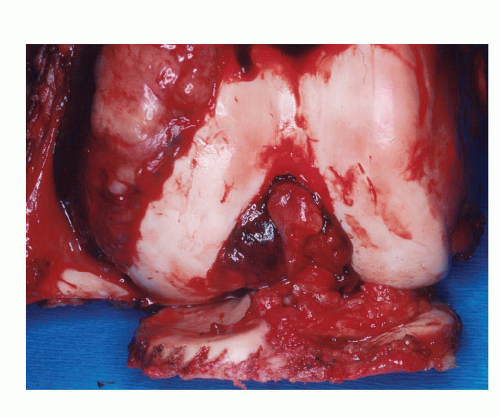 FIG 6 • Extension of an osteosarcoma of the distal femur to the knee joint along the cruciate ligaments. The articular cartilage is intact. Knee joint extension of a high-grade sarcoma of the distal femur is a rare event, necessitating extra-articular resection (ie, en bloc resection of the distal femur, knee joint, and a component of the proximal tibia) as shown here. |
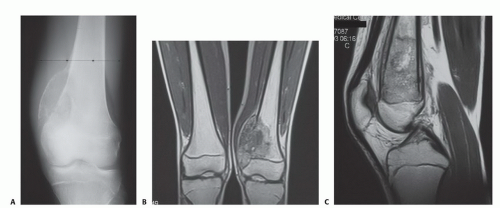 FIG 7 • Plain radiograph (A) and magnetic resonance images (B,C) showing a classical osteosarcoma of the distal femoral metaphysic breaking through the medial cortex into the adjacent soft tissues.
Related posts: Expandable Prostheses Expandable Prostheses
 Total Scapular Resections with Endoprosthetic Reconstruction Total Scapular Resections with Endoprosthetic Reconstruction
 Forequarter Amputation Forequarter Amputation
 Hip Disarticulation and Creating an Above-Knee Amputation Stump after Hip Disarticulation Hip Disarticulation and Creating an Above-Knee Amputation Stump after Hip Disarticulation
 Hamstrings Muscle Group (Posterior Thigh) Resection Hamstrings Muscle Group (Posterior Thigh) Resection
 Distal Femoral Resections with Endoprosthetic Replacement Distal Femoral Resections with Endoprosthetic Replacement
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|