Below-Knee Amputation
Daria Brooks Terrell
BACKGROUND
Extensive tumors of the distal leg, ankle, and foot often require a below-knee amputation (BKA) as the primary form of surgical treatment. With such extensive tumors in these locations, attempts at limb salvage often leave patients with a limb with very limited function. Conversely, advances in prosthetic design and engineering allow for BKA amputees to be very active in a variety of activities, often more active than patients who have had limb-sparing procedures for similar tumors.
In general, we recommend BKAs for most high-grade and many low-grade sarcomas of the foot, especially when they occur in the plantar aspect. About 1% of bone sarcomas occur in the foot; these are usually treated with a BKA (FIG 1).
ANATOMY
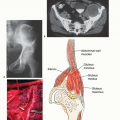
The main anatomic focus of a BKA is identification and ligation of the tibial neurovascular structures.
The anterior tibial artery and vein and deep peroneal nerve lie deep to the anterior tibialis muscle and lateral to the tibia. These structures must be identified and individually ligated.
As the dissection progresses posteriorly, the posterior tibial artery and vein and tibial nerve are found posterior to the tibia and tibialis posterior muscle and anterior to the soleus muscle.
The peroneal artery and veins also lie posterior and lateral to the tibia. They lie between the tibialis posterior and the flexor hallucis longus.
The superficial peroneal nerve is identified within the lateral compartment of the leg and also must be transected. It usually exits the fascia of the anterolateral leg approximately 12 cm proximal to the tip of the lateral malleolus. It should be identified and transected.
INDICATIONS
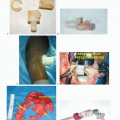
Tumor recurrence in the distal tibia, ankle, and foot not amenable to limb salvage techniques (FIG 2)
Infiltrative high-grade soft tissue sarcomas or other malignant tumors of the lower extremities
Extensive involvement of bone sarcomas of the lower extremities
Palliation
Failed attempt of radiation therapy for dorsal and plantar foot tumors
IMAGING AND OTHER STAGING STUDIES
Plain Radiography
Although plain radiographs are poor at identifying soft tissue tumors of the foot and ankle, they can be useful for the initial diagnosis of bone tumors such as enchondromas, giant cell tumors, and primary sarcomas of bone (FIG 3A).
Computed Tomography and Magnetic Resonance Imaging
Computed tomography and magnetic resonance imaging (MRI) are helpful in determining the level of intramedullary tumor involvement and the extraosseous extent of the tumor, which is used to determine the amputation level. MRI is also useful for showing tumor involvement of neurovascular structures, which often necessitates amputation (FIG 3B).
Bone Scanning
Bone scans are required if the tumor is located at or above the ankle. This study correlates well with the MRI. In general, amputation is performed 4 to 7 cm above abnormal findings on a bone scan.
Angiography and Other Studies
Angiography is very helpful in determining the extent of involvement of the anterior tibialis and posterior tibialis arteries. Tumor involvement of either of these structures determines the type of flap that should be used. This planning is important in minimizing wound healing problems.
Biopsy
As with an amputation at any level, a biopsy should be done to confirm the diagnosis before performing a BKA.
SURGICAL MANAGEMENT
The ideal level of surgical resection for a BKA is at the musculocutaneous junction of the gastrocnemius muscle. This provides better soft tissue padding and usually a more reliable blood supply for the posterior flap.
The recommended length for a BKA stump for optimal prosthetic fitting is 12.5 to 17.5 cm. However, tumor extent and margins will ultimately determine the length of the stump.
Careful flap selection is important in achieving a functional BKA stump. Because of the subcutaneous location of the tibia and sparse musculature of the anterior leg compartment, use of a long posterior flap is preferable to a fishmouth flap.
Prevention of hematoma and seroma development with the use of drains is critical. These complications can delay wound healing and, in some cases, delay adjunctive treatments such as chemotherapy and radiation therapy.
 FIG 1 • BKA is performed for malignant tumors of the distal leg, ankle, and foot. (Courtesy of Martin M. Malawer.) |
 FIG 2 • A. Locally recurrent carcinoma of the foot. This local recurrence, the patient’s fifth, occurred only a few months after the previous resection within the irradiated field. B. Extensive high-grade angiosarcoma of the dorsal aspect of the foot. (Courtesy of Martin M. Malawer.) |
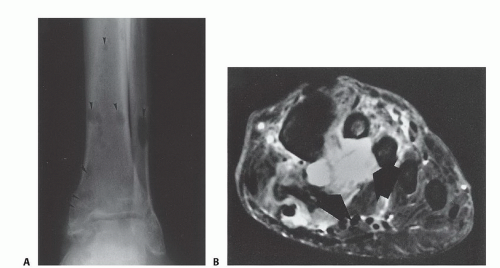 FIG 3 • A. Angiosarcomatosis of the leg and foot. There are multiple lytic lesions of the distal third of the tibia, fibula, and talus. B. T2-weighted magnetic resonance image of the foot, showing extensive high-grade malignant fibrous histiocytoma of almost the entire plantar aspect of the foot, with extension to the dorsal aspect of the foot.
Related posts: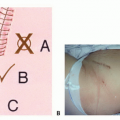 Biopsy of Musculoskeletal Tumors Biopsy of Musculoskeletal Tumors
 Overview of Resections around the Shoulder Girdle Overview of Resections around the Shoulder Girdle
 Primary and Metastatic Tumors of the Spine: Total En Bloc Spondylectomy Primary and Metastatic Tumors of the Spine: Total En Bloc Spondylectomy
 Surgical Management of Metastatic Bone Disease: Pelvic Lesions Surgical Management of Metastatic Bone Disease: Pelvic Lesions
 Adductor Muscle Group (Medial Thigh) Resection Adductor Muscle Group (Medial Thigh) Resection
 Distal Femoral Resections with Endoprosthetic Replacement Distal Femoral Resections with Endoprosthetic Replacement
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|