Axillary lymph nodes are removed for pathologic examination in patients with breast cancer to determine the presence or absence of metastatic disease; this information is essential for the purpose of cancer staging. Axillary lymph nodes may also be removed when they become enlarged due to other neoplastic diseases or as the result of various reactive and inflammatory processes. This chapter will focus on issues related to the assessment of axillary lymph nodes for the presence of metastatic breast carcinoma and other pathologic changes encountered in axillary lymph nodes.
ASSESSMENT OF LYMPH NODES FOR METASTATIC CARCINOMA
Pathologic Staging
In current clinical practice, pathologists most frequently encounter axillary lymph nodes as sentinel lymph node biopsies or in axillary dissection specimens, the latter of which are most often preceded by a sentinel lymph node biopsy. Recommendations for processing these specimens are provided in Chapter 20. The prognostic significance of axillary lymph node metastases is discussed in Chapter 10.
The examination of axillary lymph nodes from breast cancer patients requires not only assessment for the presence or absence of metastatic carcinoma but also determination of the size of the metastatic foci, if present, because this is considered in assigning the pathologic (p) N-stage. The current American Joint Commission on Cancer staging system for lymph nodes removed from patients with breast cancer is presented in Table 18.1.1 Lymph node metastases are classified as macrometastases, micrometastases, and isolated tumor cells (ITCs). Macrometastases are defined as tumor deposits >2.0 mm in size. Micrometastases (pN1mi) are deposits >0.2 mm in size and/or more than 200 cells but <2.0 mm in size. ITCs (pN0i+) are currently defined as clusters of tumor cells not exceeding 0.2 mm or nonconfluent clusters of cells not exceeding 200 cells in a single histologic lymph node cross section, detected on H&E-stained sections or by cytokeratin immunohistochemistry (Figs. 18.1 and 18.2, e-Figs. 18.1 and 18.2).1 Such deposits are usually associated with little or no stromal reaction.
TABLE 18.1 American Joint Commission on Cancer System for Pathologic Node (pN) Staging in Breast Cancer
pNX
Regional lymph nodes cannot be assessed (e.g., previously removed or not removed for pathologic study)
pN0
No regional lymph node metastasis histologically
Note: ITC clusters are defined as small clusters of cells not greater than 0.2 mm, or single tumor cells, or a cluster of fewer than 200 cells in a single histologic cross section. ITCs may be detected by routine histology or by IHC methods. Nodes containing only ITCs are excluded from the total positive node count for the purpose of N classification but should be included in the total number of nodes evaluated
pN0(i-)
No regional lymph node metastasis histologically, negative IHC
pN0(i+)
Malignant cells in regional lymph node(s) not greater than 0.2 mm (detected by H&E or IHC including ITC)
pN0(mol-)
No regional lymph node metastases histologically, negative molecular findings (RT-PCR)
pN0(mol+)
Positive molecular findings (RT-PCR), but no regional lymph node metastases detected by histology or IHC
pN1
Micrometastases or metastases in one to three axillary lymph nodes and/or in internal mammary nodes with metastases detected by sentinel lymph node biopsy but not clinically detected
pN1mi
Micrometastases (greater than 0.2 mm and/or more than 200 cells, but none >2.0 mm)
pN1a
Metastases in one to three axillary lymph nodes; at least one metastasis greater than 2.0 mm
pN1b
Metastasis in internal mammary nodes with micrometastases or macrometastases detected by sentinel lymph node biopsy but not clinically detected
pN1c
Metastases in one to three axillary lymph nodes and in internal mammary lymph nodes with micrometastases or macrometastases detected by sentinel lymph node biopsy but not clinically detected
pN2
Metastases in four to nine axillary lymph nodes or in clinically detected internal mammary lymph nodes in the absence of axillary lymph node metastases
pN2a
Metastases in four to nine axillary lymph nodes or in clinically detected internal mammary lymph nodes in the absence of axillary lymph node metastases
pN2b
Metastases in clinically detected internal mammary lymph nodes in the absence of axillary lymph node metastases
pN3
Metastases in 10 or more axillary lymph nodes; or in infraclavicular (level III axillary) lymph nodes; or in clinically detected ipsilateral internal mammary lymph nodes in the presence of one or more positive level I/II axillary lymph nodes; or in more than three axillary lymph nodes and in internal mammary lymph nodes with micrometastases or macrometastases detected by sentinel lymph node biopsy; or in ipsilateral supraclavicular lymph nodes
pN3a
Metastases in 10 or more axillary lymph nodes (at least one tumor deposit >2.0 mm) or metastases to the infraclavicular (level III axillary) lymph nodes
pN3b
Metastases in clinically detected ipsilateral internal mammary lymph nodes in the presence of one or more positive axillary lymph nodes or in more than three axillary lymph nodes and in internal mammary lymph nodes with micrometastases or macrometastases detected by sentinel lymph node biopsy but not clinically detected
pN3c
Metastasis in ipsilateral supraclavicular lymph nodes
Adapted from AJCC Cancer Staging Manual Seventh Edition. New York, NY: Springer; 2010.
Unfortunately, in some cases, determining the size of a lymph node metastasis, and in turn the pN-stage, is problematic and subject to considerable interobserver variability.2, 3 and 4 In particular, how to categorize lymph nodes that contain multiple foci of ITC/small tumor cell clusters has been a matter of debate. Some pathologists assign the pN-stage based on the size of the single largest cell cluster; if it is ≤0.2 mm, the patient is staged as pN0(i+) even if there are numerous aggregates in that size range. Others measure the span of aggregates that are in close proximity to each other and consider that to represent the size of the metastatic deposit (Fig. 18.3). The current edition of the staging system1 recommends that when there are multiple foci of tumor cells in a lymph node, the size of only the largest contiguous tumor deposit is used to classify the node; the sum of all the individual tumor deposits or the distance between non-contiguous deposits should not be used. In the case of a lymph node that contains dispersed ITC or small aggregates throughout the subcapsular and/or medullary sinuses (as is commonly seen in invasive lobular carcinomas), some would consider the pathologic nodal stage pN0(i+). However, most would consider the entire node to be involved and stage it as a macrometastasis (pN1a) if the node itself was >2.0 mm in size (Fig. 18.4). The histologic finding of extension of tumor cells beyond the lymph node capsule into the perinodal soft tissue (extranodal or extracapsular extension) does not change the pathologic N-stage, but should be commented on in the surgical pathology report because it may represent a risk factor for tumor recurrence (Fig. 18.5).
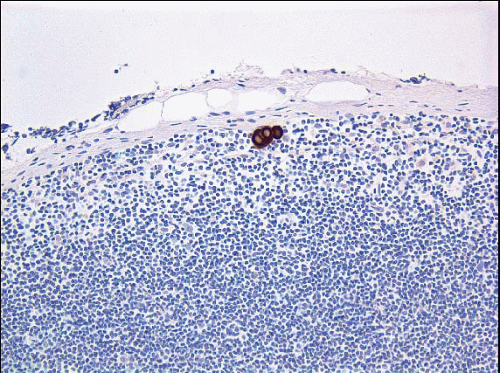
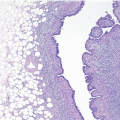
FIGURE 18.1 Isolated tumor cells in the subcapsular sinus of a sentinel lymph node, detected by cytokeratin immunostain. If this were the only finding in the lymph nodes, the pathologic node stage would be pN0(i+).
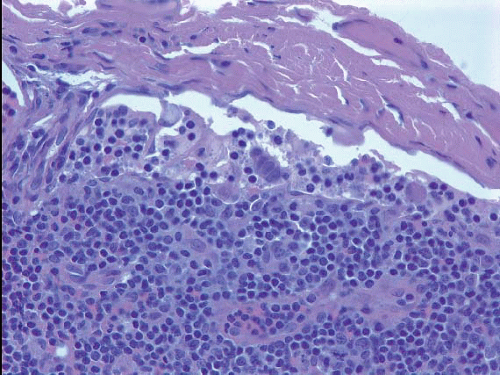
FIGURE 18.2 Isolated tumor cells in the subcapsular sinus of a sentinel lymph node detected on an H&E-stained section. If this were the only finding in the lymph nodes, the pathologic node stage would be pN0(i+).
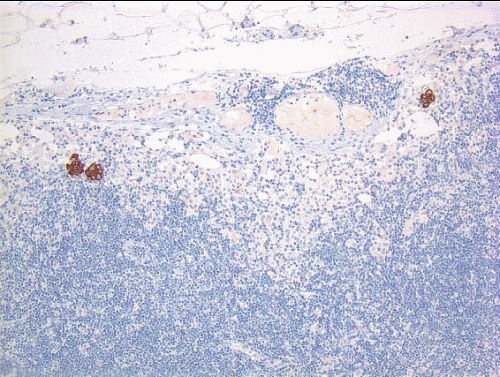
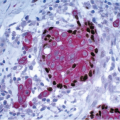
FIGURE 18.3 Several isolated tumor cell clusters detected on a cytokeratin immunostain. Some observers would consider this lymph node to be involved by isolated tumor cells; others would measure the distance from one cluster to the other and use that size to determine the category of lymph node stage. In current practice, a lymph node with these features should be staged as pN0(i+).
As indicated in Chapter 20, evaluation of sentinel lymph nodes by frozen sections and/or cytologic preparations is performed at some institutions to determine the need for further axillary node dissection at the time of sentinel lymph node biopsy.5 It should be noted that regardless of the method used for intraoperative evaluation, the false-negative rate is approximately 25% to 30%. Therefore, the final pathologic nodal stage can only be determined after examination of permanent sections. Further, as discussed in Chapter 20, results from the American College of Surgeons Oncology Group (ACOSOG) Z0011 trial have called into question the need for routine intraoperative evaluation of sentinel lymph nodes.6
Histologic Features of Lymph Node Metastases
Breast cancer metastases in axillary lymph nodes almost always have cytoarchitectural and immunophenotypic features similar to those of the primary tumor. Differences in the histologic appearance between the tumor in the lymph nodes and that in the breast should raise the possibility of another, undetected area of carcinoma in the breast. Occasionally, metastatic carcinoma in a lymph node occurs in circumscribed nests, which may show foci of necrosis creating an appearance reminiscent of ductal carcinoma in situ (DCIS) (Fig. 18.6).
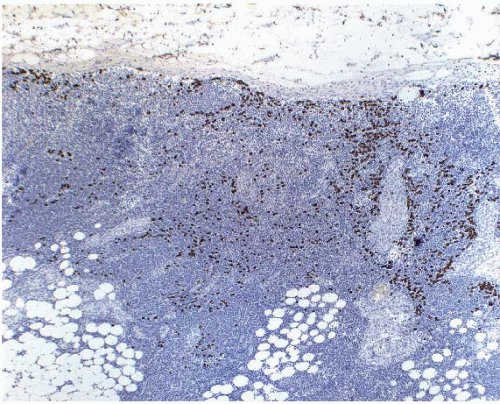
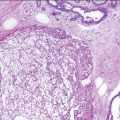
FIGURE 18.4 Sentinel lymph node from a patient with invasive lobular carcinoma, immunostained for cytokeratin showing numerous cytokeratin-positive tumor cells throughout the node. Although this could theoretically be staged as pN0(i+), it is better considered to be pN1a (Courtesy of Dr. Susan Lester).
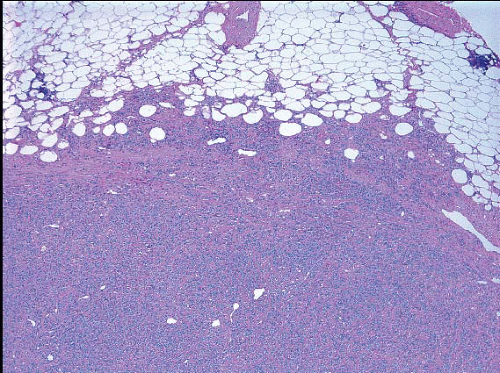
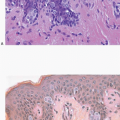
FIGURE 18.5 Metastatic lobular carcinoma in axillary lymph node with extracapsular extension of tumor into perinodal adipose tissue.
FIGURE 18.6 Metastatic carcinoma in axillary lymph node. Some of the metastatic tumor cell nests have a pattern that mimics ductal carcinoma in situ.
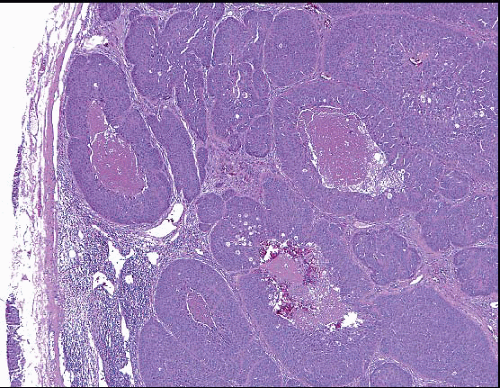
Macrometastases disrupt the nodal architecture and are readily recognizable on low-power microscopic examination, if not grossly (Fig. 18.7). However, recognition of smaller metastatic foci may be more problematic. As is the case for carcinomas metastatic to lymph nodes in general, the earliest breast cancer metastases in axillary lymph nodes usually appear in the subcapsular sinus followed by the medullary sinuses; careful scrutiny of these regions is essential in cases in which metastases are not immediately evident. Further, tumor cells in the sinuses must be distinguished from histiocytes. This may be especially difficult in patients with invasive lobular carcinoma, the cells of which may appear deceptively bland (Fig. 18.8
Only gold members can continue reading. Log In or Register to continue