Guideline
LDL-C mmol/l
Non-HDL-C
apoB
Concentration mmol/l mg/dl
NHANES Population percentile
Concentration mmol/l mg/dl
NHANES population percentile
Concentration g/l
NHANES population percentile
National Lipid Association 197
High risk
< 2,6 < 100
33%
< 3,4 < 130
42%
Very high risk
< 1,8 < 70
8%
< 2,6 < 100
16%
ACC/AHA 223
High risk
< 2,6 < 100
33%
< 3,4 < 130
42%
< 0,9
51%
Very high risk
< 1,8 < 70
8%
< 2,6 < 100
16%
< 0,8
35%
EAS/ESC 194
High risk
< 2,6 < 100
33%
< 3,4 < 130
42%
< 1,0
67%
Very high risk
< 1,8 < 70
8%
< 2,6 < 100
16%
< 0,8
35%
Joint British Society 3 196
High risk and Very high risk
< 2,0 < 77
12%
< 3,0 < 115
27%
Canadian Cardiovascular Society 195
High risk and very high risk
< 2,0 < 77
12%
< 2,6 < 100
16%
< 0,8
35%
EAS-HTG treatment target 197a
High risk
< 0,8
35%
Very high risk
< 0,7
19%
All these approaches have been criticized by the ACC/AHA guidelines223 on the grounds that the major statin trials actually tested regimens, not targets, and therefore all patients should receive the same standard dose of statin without adjustment based on any measure of LDL. This No Target/Regimen Only approach is diametrically opposed to the target strategies but is also evidence-based, actually, paradoxically, on the same evidence on which the target strategies are based. Because therapy is one of the most important issues we deal with, we must try to understand the relative strengths and weaknesses of these two different treatment strategies for LDL lowering. Based on this analysis, we will present the option we prefer – the apoB two-step approach, which we believe is the most clinically and physiologically appropriate approach given all the evidence and the limitations in the evidence.
6.2 LDL Lowering Treatment Strategies
6.2.1 The No-Target/ Regimen Only-based Approach
The No-Target/Regimen Only approach states that the routine clinical regimen should be the regimen that was used in successful clinical trials. Clinical trials, the argument goes, tested regimens, not target levels and, therefore, it is regimens not targets that were validated by the clinical trials.224 Moreover – the argument continues – lowering of LDL may not be the only mechanism of benefit from statins. Any of a number of other possible effects, such as reduction of inflammation, might be responsible for the so-called pleotropic clinical benefits of statins – that is, all the putative mechanisms other than LDL lowering that might produce clinical benefit by statins. Therefore, changes in LDL are not the only index of the therapeutic effects of statins from which it follows that changes in LDL should not govern the dose of statins. The premise for the argument is logical, but is the evidence for it complete and compelling?
The answer, unfortunately, is no. Amongst our reservations, the first is that six therapeutic trials – TNT,225 GREACE,226 AFCAPS/TexCAPS,227 PROVE-IT TIMI,225 MEGA228and Post-CABG229 – did select doses in order to achieve a prespecified level of LDL. The number is not trivial and while the design of most as target trials may not be ideal and the evidence is incomplete, it is not non-existent.
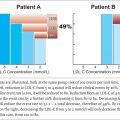
Second, not all patients benefit equally, either clinically or in terms of LDL lowering, from the same dose of a statin. This distinction between individual and group benefit has been largely overlooked and that is unfortunate. The Cholesterol Treatment Trialists (CTT) meta-analysis of the cholesterol-lowering trials230 concluded that the lowering of clinical events by a constant decrease in LDL-C is constant: that is, 1 mmol/l (38.5 mg/dl) reduction of LDL-C reduced clinical events by approximately 20%. Based on this finding, many have concluded that the relative benefit of statins is the same in all and the absolute benefit is determined by the absolute risk. In other words, all individuals are the same and the group response applies, therefore, to all.
But this conclusion does not follow from the CTT findings. If the relative benefit per mmol/l lowering of LDL-C is constant, then the absolute benefit possible depends on the baseline level of LDL-C because with each mmol/l reduction in LDL-C, risk is reduced by 20% from baseline. Thus, while the relative benefit per mmol/l lowering of LDL-C is constant, the absolute benefit depends on the baseline level of LDL-C.231 Moreover – and this point also seems to have been overlooked – the absolute lowering of LDL-C by a statin depends not only on the dose and potency of the statin but also on the baseline level of LDL: the higher the baseline value, the greater the drop. It is the relative decrease in LDL produced by a statin that is constant not the absolute decrease.232 Since, as we have just shown, benefit correlates with the absolute decrease in LDL, there will be greater benefit from the same dose and potency of a statin with higher baseline levels of LDL. Thus, it follows, logically and directly, from the CTT results230 that not all patients benefit equally from statin therapy: those with higher levels achieve greater absolute benefit compared with those with lower levels (see Figure 7.4 ). Absolute benefit is meaningful clinically. Relative benefit can be misleading as the Guideline recommendations demonstrate. Unfortunately, this point is not widely appreciated.
Related posts:
 Secondary ApoB Dyslipoproteinemias
Secondary ApoB Dyslipoproteinemias
 ApoB in Cardiovascular Risk Prediction
ApoB in Cardiovascular Risk Prediction
 The Future of ApoB: Moving from the Risk Prediction Paradigm to the Causal Exposure Paradigm
The Future of ApoB: Moving from the Risk Prediction Paradigm to the Causal Exposure Paradigm
 Diagnosis of the ApoB Dyslipoproteinemias: The ApoB Algorithm
Diagnosis of the ApoB Dyslipoproteinemias: The ApoB Algorithm
 The Primary ApoB Dyslipoproteinemias
The Primary ApoB Dyslipoproteinemias
 The Life History of ApoB Lipoprotein Particles
The Life History of ApoB Lipoprotein Particles
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


