Although benign hemangiomas are among the most common diagnoses among connective tissue tumors, angiosarcomas and other sarcomas arising from blood vessels are rare, even among sarcomas. Because endothelial tumors have unique embryonal derivation compared with other sarcomas, it is not surprising they have unique characteristics. Herein are reviewed some of these unique characteristics and therapeutic options for patients with some of these diagnoses, highlighting the potential of new agents for these tumors, which will in all likelihood also impact treatment on more common cancers.
Key points
- •
Vascular sarcomas are rare and collectively affect fewer than 600 people a year in the United States (incidence approximately 2/million).
- •
Because angiosarcomas, hemangioendotheliomas, and other vascular tumors have unique embryonal derivation, it is not surprising that they have a unique sensitivity pattern to chemotherapy agents.
- •
Surgery, when possible, remains the primary treatment for angiosarcomas.
- •
Adjuvant radiation for primary disease seems prudent for at least some angiosarcoma, given the high local-regional recurrence rate of these tumors. Angiosarcomas also have a high rate of metastasis, but it is not clear that adjuvant chemotherapy improves survival.
- •
Epithelioid hemangioendothelioma is a unique form of sarcoma often presenting as multifocal disease. Most patients can do well with observation alone, although a fraction of patients have more aggressive disease and have difficulties in both local control and metastatic disease.
- •
Anthracyclines, alkylating agents such as ifosfamide, are active against at least some vascular sarcomas. Angiosarcomas demonstrate a unique sensitivity to taxanes, and gemcitabine, vinorelbine, and vascular endothelial growth factor (VEGF) or vascular endothelial growth factor receptors (VEGFR) antagonists all have at least some activity against these tumors.
- •
New targets to consider for therapy include angiopoietin antagonists as well as inhibitors notch or ephrin signaling pathways.
Introduction
Of the 14,000 cases of sarcoma diagnosed in the United States annually, sarcomas arising from endothelium and other elements of blood vessels constitute ∼2% to 3%, and thus it is likely that fewer than 600 people in the United States are affected each year. This fact is surprising, given the common nature of the benign counterpart of these tumors, hemangiomas, arteriovenous malformations, and other lesions in the population.
In this review, examined are some of the unique characteristics and therapeutic options for patients with tumors that arise from endothelium or its precursors, highlighting the potential of new agents for these tumors. Given the activity of anti-angiogenic therapy in both vascular sarcomas and other cancers, new agents will have an impact on both vascular sarcomas and more common cancers.
Introduction
Of the 14,000 cases of sarcoma diagnosed in the United States annually, sarcomas arising from endothelium and other elements of blood vessels constitute ∼2% to 3%, and thus it is likely that fewer than 600 people in the United States are affected each year. This fact is surprising, given the common nature of the benign counterpart of these tumors, hemangiomas, arteriovenous malformations, and other lesions in the population.
In this review, examined are some of the unique characteristics and therapeutic options for patients with tumors that arise from endothelium or its precursors, highlighting the potential of new agents for these tumors. Given the activity of anti-angiogenic therapy in both vascular sarcomas and other cancers, new agents will have an impact on both vascular sarcomas and more common cancers.
Scope of the diagnoses discussed
The World Health Organization (WHO) fascicle for soft tissue sarcomas was updated in 2013. The terminology for soft tissue vascular sarcomas is largely unchanged from the prior 2002 version. For bone vascular tumors, changes are anticipated to make terminology for both groups of vascular tumors more consistent. Technically, leiomyosarcoma could be considered vascular sarcomas, because they frequently arise from branches of veins, presumably from smooth muscle cells of blood vessels or their precursors, but they are not discussed here. For space considerations, also not addressed are other tumors that arise from other cellular structures associated with blood vessels (eg, solitary fibrous tumor or intimal sarcoma, each of which has unique biology and sensitivity to systemic therapeutics as well). Finally, there are also vascular components of other tumors such as angiomyolipoma, but these are also not discussed in this review.
Demographics
Kaposi sarcoma (KS) is an AIDS (acquired immune deficiency syndrome)-defining diagnosis and happily has been observed less frequently, with the advent of newer generations of anti-retroviral therapy for people with human immunodeficiency virus (HIV) infections. KS also arises in approximately 1 in 200 patients with organ transplants due to immunosuppressive drugs. KS is also seen in an endemic form in patients from the Mediterranean basin and endemically in Africa and the Mideast as well. In the United States, what was a rare cancer became common with the advent of AIDS, with a peak incidence of 10 to 20/1000 HIV-positive patients per year in the United States, but an ∼80% decrease with the broad use of multitargeted anti-retroviral therapy. Nonetheless, KS remains more common than other vascular sarcomas.
Angiosarcoma may arise in any part of the body but is more common in soft tissue than in bone. The peak age of incidence seems to be the 7th decade, and men are affected more than women. The head and neck area is probably the most common site of diagnosis, and the most common site of radiation-induced angiosarcoma development is the breast. With an increasing incidence of breast cancer, an increase in angiosarcoma of the breast has also been observed with a cumulative incidence of 0.9 per 1000 breast cancer cases over 15 years. The median latency is 4 to 8 years after treatment.
In addition, it is worth noting that after rhabdomyosarcoma, angiosarcoma is likely the second most common sarcoma to arise from germ cell tumors. In all, angiosarcoma and epithelioid hemangioendothelioma (EHE) represent under 2% to 3% of all sarcoma diagnoses.
Epithelioid hemangioendothelioma (EHE) is substantially less common than angiosarcoma, but given the more indolent nature of the tumor, there is a relatively larger prevalent population. It occurs in a younger population, with a peak incidence in the 4th to 5th decade. Women seem to be affected more commonly than men. In a survey of EHE patients from an EHE support group, overall survival was 73% at 5 years.
Angiogenesis versus vasculogenesis and the growth of endothelial tumors
There is significant confusion in the literature regarding the terms vasculogenesis and angiogenesis. Vasculogenesis typically has been a term applied to de novo blood vessel formation during embryonic development. Conversely, classically, angiogenesis was described to be the formation of new capillaries by sprouting or splitting of preexisting vessels. In common oncological parlance today, angiogenesis is used to describe the growth of any new blood vessel of any size. It has been proposed that capillarogenesis is a more accurate term to describe the “universal formation of new capillaries, during development and in the adult, without any implications regarding possible underlying mechanisms, processes, or the cells that give rise to this outcome” and distinguishable from the growth and maturation of these smallest of vessels into larger ones.
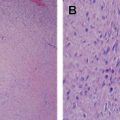
Clearly, KS, angiosarcomas, and hemangioendotheliomas fall into the categories of tumors of endothelial cells or their precursors. Clinicians see both nodular masses and superficial spreading versions of endothelial tumors ( Fig. 1 ). Pathologists have described some microscopic features of cutaneous angiosarcomas as having areas that are more solid (which one can hypothesize as being local aggressiveness of the tumor) as well as a characteristic dissecting pattern among existing collagen bundles, which could be construed as an aberrant version of capillarogenesis. These features seem to correlate with the gross pictures of tumor growth. The dissecting features may also account for the very common marginal recurrence of these tumors after primary resection. The authors further hypothesize that the multifocal pattern of these tumors, seen in particular in some versions of EHE, may arise from an unusual pattern of self-seeding as described by Comen and colleagues and Kim and colleagues.

Like angiosarcoma, KS is described as evolving between a patch stage, a plaque stage, and frankly nodular disease, again harkening to the pattern of growth seen in other endothelial tumors in which aberrant capillarogenesis is involved.
Cause of sarcomas of endothelial origin
The most common cause of angiosarcoma seems to be therapeutic radiation, which was a well-recognized cause of hepatic angiosarcoma in the era when the thorium-containing contrast agent Thorotrast was used. Presently, the breast is the most common anatomic site affected by radiation-induced angiosarcoma, raising the question of the use of lumpectomy and radiation for ductal carcinoma in situ, a noninvasive form of breast cancer in which this recommendation is often made in lieu of wide surgical resection.
Angiosarcomas also arise after exposure to vinyl chloride, although they remain rare tumors even in an exposed population. Angiosarcomas are also observed after lymphedema from any cause, be it surgical, filarial, or congenital, and carries the term Stewart-Treves syndrome from the pathologists who first described it.
Whether arising in its epidemic HIV-associated form or endemic form, KS is caused by human herpesvirus-8 (HHV8), a γ-2 herpesvirus also termed Kaposi sarcoma herpesvirus. HHV8 functions at least in part through stimulation of chemokines, a viral version of interleukin-6, and anti-apoptotic proteins for its growth and transmission. The role of microRNA networks in its propagation as well as change from latent to lytic state is under scrutiny.
Genetic changes in endothelial-based sarcomas
Specific sarcomas of endothelial derivation are described in Table 1 , along with genetic alterations observed for each subtype. The specifics of HHV8 biology are beyond the scope of this review, but point to specific genes that may be important in the conversion of an endothelial cell to a sarcoma cell, for example, cyclin D homologues and a G-protein-coupled receptor. Also not discussed here are the very interesting findings with respect to genetic knockout mice and vascular development; arteriovenous malformations arise in several of these mice and understanding of these pathways could affect therapy for patients with vascular sarcomas.
| Histology | Characteristic Genetic Changes/etiology |
|---|---|
| Kaposi sarcoma | HHV-8/Kaposi sarcoma herpesvirus |
| Angiosarcoma | MYC amplification (in radiation-induced angiosarcoma more than primary angiosarcoma) KDR/VEGFR2 mutations, FLT4/VEGFR3 amplifications (frequency well under 50%) |
| Epithelioid hemangioendothelioma | t(1;3) (p36.3;q25) WWTR1-CAMTA1 (more common) t(X;11) (p11.23;q22.1) YAP1-TFE3 |
| Pseudomyogenic hemangioendothelioma | t(7;19) (q22;q13); frequency unknown |
Angiosarcomas are largely aneuploid tumors, which for at least some of them makes sense, given their association with therapeutic irradiation. Because there are only rare cases of angiosarcomas that seem to arise from a benign lesion such as a hemangioma, the pathway leading to the 2 types of vascular lesions seems distinct, although clearly a genetic examination of such rare compound lesions would be of great interest to understand angiosarcomagenesis. ERG (ETS [E twenty six]-related gene) is overexpressed in most angiosarcomas as well as other benign and malignant vascular tumors and seems to be a consistent endothelial lineage marker. MYC amplification seems to be more common in secondary than primary angiosarcomas. miR17-92 seems to be up-regulated with MYC in radiation-induced angiosarcomas as well, with concurrent downregulation of anti-angiogenic gene THBS1. KDR mutation and FLT4 amplification have been observed in a fraction of angiosarcomas. There does not sem to be a correlation between mutation status and outcome with vascular endothelial growth factors (VEGFs).
EHE has been found to be associated with the t(1;3) (p36.3;q25) WWTR1-CAMTA1 translocation, and less commonly t(X;11) (p11.23;q22.1) YAP1-TFE3. WWTR1 , also called TAZ , is a gene involved in 14-3-3 transcriptional factor activation and signaling in the hippo pathway that is normally highly expressed in endothelial cells. CAMTA1 is part of a family of calmodulin-binding transcription activators, normally found only in brain. YAP1 is another gene in the hippo pathway, thus closely EHE to hippo signaling in all cases examined to date. These fusions are not directly targetable with present day therapeutics but may reveal downstream targets. Of note, the multiple lesions examined from a single patient all seem to have the same translocation, providing evidence that this is a matter of tumor metastasis or self-seeding at an early stage of development.
Pathologic abnormality of endothelial tumors
All angiosarcomas are presently considered high-grade neoplasms, regardless of degree of vascular differentiation or cytology, save primary breast angiosarcomas, where the Rosen 3-tier grading scheme is used. The concept angiosarcoma grading was challenged in one analysis of what was largely consultation material. In this study of 49 patients Rosen grade was not prognostic, in keeping with outcomes from other primary sites of disease.
As noted above, angiosarcomas demonstrate a dissecting pattern of blood vessel formation and bear the endothelial markers characteristic of this cell lineage. There are variations of the histology based on anatomic site, with cutaneous lesions demonstrating dissecting and solid patterns of growth, and some tumors of visceral origin more commonly displaying epithelioid features. In comparison to benign lesions, areas with multilayered endothelial growth are characteristic of angiosarcoma, and there is at least some evidence of cytologic atypia. Mitotic rate is variable, but greater than that seen for hemangiomas.
Immunohistochemical markers for angiosarcoma include CD31, ERG, and CD34, among others. Although FLT4/vascular endothelial growth factor receptor3 was proposed as a lymphatic-specific marker based on in situ hybridization in developing mice, a significant number of angiosarcomas express one or more lymphatic markers, without direct correlation with FLT4 gene amplification. It is hoped that work on the association of ephrin B2 and EphB4 expression in arterial versus venous development will shed some light on this fundamental issue regarding the nature of these tumors.
EHE are characterized by endothelial cells arranged in single files, nest, or more solid growth, and distinct lack of vessel formation that is characteristic of angiosarcomas. Intracytoplasmic vacuoles are often seen, and some of these may have red blood cells in them as well. Like angiosarcomas, EHE are positive for CD31, CD34, and ERG, and often are keratin positive.
KS usually shows a greater number of spindle-shaped cells than angiosarcoma and also forms vascular channels containing red blood cells, like angiosarcoma. Lymphoplasmacytic infiltrates may be observed. Eosinophilic hyaline inclusions can be observed in more advanced lesions. Although CD31 and CD34 immunohistochemicals are also common in KS, HHV8 latent nuclear antigen-1 is only positive in KS and not in the other diagnoses.
The 2013 WHO classification adds the unifying entity pseudomyogenic hemangioendothelioma, which has also been called epithelioid sarcoma-like hemangioendothelioma. It will be included in the “rarely metastasizing” category of the WHO soft tissue sarcoma classification. Like EHE, it can be multifocal, and at least some cases are associated with a t(7;19) (q22;q13) translocation, distinct from other forms of hemangioendothelioma described above. There are presently no data regarding chemotherapy sensitivity of this unique vascular sarcoma subtype.
Primary therapy
Kaposi Sarcoma
For KS, observation alone, in particular in someone with improving CD4 counts after the institution of anti-retroviral therapy, seems prudent except for those patients with obvious symptoms. For transplant-related KS patients cautious decrease or withdrawal of immunosuppressive therapy is often effective, but this benefit comes at the risk of allograft rejection. The switch of the immunosuppressive regimen from calcineurin inhibitors to target rapamycin inhibitor sirolimus has been reported to induce significant regression of KS lesions.
KS lesions are usually not isolated, and thus “primary therapy” takes on a different tone. Intralesional chemotherapy such as vinblastine can be used for symptomatic isolated lesions, as can topical retinoids. Radiation therapy is usually used as primary therapy disease that is symptomatic and too extensive to treat with more localized treatments.
Angiosarcoma and EHE
When feasible, primary treatment of angiosarcoma or EHE is surgical. However, for the relatively common site of head and neck it is not uncommon to encounter unresectable disease that covers too large an area of the scalp to treat surgically, in which case electron beam radiation sometimes can be used for local control. In the situation of radiation-induced angiosarcoma of the breast, the local recurrence risk of these lesions highlights the need for resection of irradiated parenchyma and skin as primary therapy to attempt to improve the local control rate.
For primary therapy of EHE or angiosarcoma involving the liver, embolization can be useful, taking advantage of the differences between tumor and normal tissue tolerance for hypoxia. Shamefully, there remain no comparative data on chemoembolization versus bland embolization, despite thousands of patients with a variety of diagnoses being treated with either modality.
After primary therapy for angiosarcoma (or potentially EHE in the correct anatomic location), general principles regarding adjuvant therapy in sarcoma apply, with some caveats. If an angiosarcoma was caused by radiation, it is oftentimes not possible to administer adjuvant radiation. In some cases a way to boost local doses of radiation can be considered, such as brachytherapy, but these are considered on a case-by-case basis.
In terms of adjuvant chemotherapy, the low response rate to chemotherapy in EHE makes it a relatively unattractive prospect. In addition, the small number of people with localized disease with EHE at presentation makes this clinical situation uncommon.
As for adjuvant chemotherapy for angiosarcoma, meta-analysis data indicate that patients with unselected sarcomas have a survival benefit from ifosfamide-based chemotherapy. However, for the few positive individual studies over the last few decades of adjuvant therapy in soft tissue sarcomas, there are multiple negative individual studies, including the largest such randomized study, making the recommendation of adjuvant anthracycline-ifosfamide a difficult decision. As with all clinical decision-making in which there are conflicting data, decisions should be made on a patient-by-patient basis.
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


