This article outlines the anesthetic management of patients undergoing cytoreductive surgery with hyperthermic intraperitoneal chemotherapy. This includes a discussion of preoperative evaluation, hemodynamic monitoring, fluid and electrolyte therapy, and temperature management. An understanding of the unique physiologic consequences of this procedure is essential to ensure good outcomes and avoid patient injuries.
- •
Cytoreductive surgery with hyperthermic intraperitoneal chemotherapy (HIPEC) is an extensive, invasive procedure that presents unique physiologic challenges.
- •
During the HIPEC portion of the surgery, patients develop a hyperdynamic state.
- •
A balanced approach to fluid management, which incorporates both crystalloids and colloids, is encouraged.
- •
Hemodynamic monitoring with estimation of cardiac output is useful for optimizing organ perfusion while preventing fluid overload.
- •
To avoid renal injury by chemotherapeutic agents, urine output should be maintained at a high rate during that phase of the procedure.
- •
Thoracic epidural anesthesia improves analgesia and facilitates early mobilization of patients.
Introduction
Cytoreductive surgery with hyperthermic intraperitoneal chemotherapy (HIPEC) plays an increasingly important role in the management of patients with a variety of malignancies. These complex procedures subject patients not only to the usual physiologic challenges associated with major surgery, but also to the thermal stress induced by the intraperitoneal instillation of heated chemotherapeutic solution. The surgery is complex, and not without complications. Safety is therefore the primary goal. The formation of a specialized team, with close communication among anesthesia providers and surgical staff, enhances patient outcomes. This article outlines an approach that has evolved over the past 6 years in more than 500 patients at our center, and provides an overview of the management of the surgical patient during the HIPEC procedure.
Preoperative evaluation
In addition to the usual preoperative evaluation of patients undergoing major abdominal surgery, special attention should be paid to a few conditions that may present additional challenges for the anesthesia provider. A thorough preoperative airway evaluation should be performed to avoid unexpected difficulty. Patients may have significant abdominal distention because of various combinations of tumor, mucus, and ascites; 10 to 15 L of pathologic fluid accumulation may be present. Increased abdominal volume and pressure decreases functional residual capacity, predisposing patients to both rapid oxygen desaturation and aspiration of gastric contents after induction of anesthesia.
Cardiac Risk
Because induced hyperthermia results in increased myocardial oxygen demand, patients with preexisting coronary artery disease, heart failure, or other cardiac pathology may be at risk for hemodynamic decompensation. Similarly, patients with depressed left ventricular function may not be able to tolerate aggressive intraoperative volume therapy, which may precipitate pulmonary edema. For these reasons, cytoreductive surgery with HIPEC should be considered as a procedure that presents elevated cardiac risk. For patients with known cardiac disease or other risk factors, preoperative cardiac evaluation per American Heart Association guidelines is recommended.
Preoperative evaluation
In addition to the usual preoperative evaluation of patients undergoing major abdominal surgery, special attention should be paid to a few conditions that may present additional challenges for the anesthesia provider. A thorough preoperative airway evaluation should be performed to avoid unexpected difficulty. Patients may have significant abdominal distention because of various combinations of tumor, mucus, and ascites; 10 to 15 L of pathologic fluid accumulation may be present. Increased abdominal volume and pressure decreases functional residual capacity, predisposing patients to both rapid oxygen desaturation and aspiration of gastric contents after induction of anesthesia.
Cardiac Risk
Because induced hyperthermia results in increased myocardial oxygen demand, patients with preexisting coronary artery disease, heart failure, or other cardiac pathology may be at risk for hemodynamic decompensation. Similarly, patients with depressed left ventricular function may not be able to tolerate aggressive intraoperative volume therapy, which may precipitate pulmonary edema. For these reasons, cytoreductive surgery with HIPEC should be considered as a procedure that presents elevated cardiac risk. For patients with known cardiac disease or other risk factors, preoperative cardiac evaluation per American Heart Association guidelines is recommended.
Intraoperative management
Induction
As previously noted, many patients presenting for HIPEC surgery are at risk for both oxygen desaturation and aspiration of gastric contents. Accordingly, rapid sequence induction is the preferred approach in this setting. In our institution, videolaryngoscopy is commonly used as a first-line technique for endotracheal intubation, and has greatly simplified airway management, even in the setting of anticipated difficult intubation. Meticulous attention to patient positioning and padding of potential pressure sites is performed to decrease the risk of injury during these frequently lengthy procedures.
Hemodynamic Monitoring
In addition to routine monitors, a radial arterial line is placed for both hemodynamic monitoring and blood gas analysis. Our group, however, has recently reconsidered the necessity and utility of central venous monitoring. Central venous and pulmonary artery pressures are static measures, which do not accurately reflect volume status or volume responsiveness. Furthermore, central venous lines expose patients to potential mechanical injury and serious infection, and are a well-recognized source of risk to patients undergoing HIPEC. The routine placement of central venous lines, therefore, is no longer performed at our institution, unless indicated for vascular access.
Concerns regarding the safety and utility of invasive hemodynamic monitoring have spurred interest in less-invasive solutions. More recently, our group has used both minimally invasive pulse contour analysis (LiDCO Rapid, LiDCO, Ltd, Cambridge, England) and noninvasive bioreactance devices (NICOM, Cheetah Medical, Tel Aviv, Israel) for hemodynamic monitoring.
Pulse contour analysis monitoring has been previously described in the setting of HIPEC surgery. Analysis of the arterial waveform obtained via a pressure transducer is used to generate estimates of stroke volume and cardiac output. The NICOM (noninvasive cardiac output monitor) uses 2 pairs of electrodes placed around the heart to transmit and receive a 75-kHz signal placed across the thorax. Phasic blood flow in the descending thoracic aorta results in changes in reactance (the combined effect of inductance and capacitance) and phase angle shifts in the received signal. The electrical changes caused by aortic blood flow are translated using a computer algorithm to yield real-time estimates of stroke volume and cardiac output.
Both pulse contour and bioreactance estimates of cardiac output have acceptable clinical accuracy compared with pulmonary artery catheter, and may in fact be more responsive to sudden changes in loading conditions. The accuracy of pulse contour analysis, however, may be impaired in patients with septic shock, vasoconstriction, or vasodilation, as changes in peripheral arterial tone may not reflect changes in aortic blood flow.
Beat-to-beat changes in stroke volume induced by positive-pressure ventilation can be used as an estimate of volume responsiveness. In the normal heart, positive-pressure ventilation causes changes in preload, which are exaggerated in the setting of hypovolemia. Stroke volume variation (SVV) in the 12% to 13% range may reflect volume responsiveness. Low stroke volume variation usually signifies euvolemia; however, there is substantial technical heterogeneity among the available hemodynamic monitors, and the true significance of elevated SVV may be questionable in some cases. In some studies, pulse-pressure variation has been a more reliable indicator of preload responsiveness that SVV. Additionally, patients with impaired systolic function tend to be more afterload than preload dependent, and may not exhibit increased stroke volume variability in the setting of hypovolemia. With the aforementioned caveats, the addition of dynamic measures of cardiac performance has enabled so-called goal (or flow) directed fluid therapy.
Management During Chemotherapy Infusion
Unique aspects of HIPEC surgery include hemodynamic alterations owing to induced hyperthermia, as well as the potential for nephrotoxicity secondary to the use of chemotherapeutic agents. Appropriate management of intravenous fluid therapy is critical for maintaining optimal end-organ perfusion, and avoiding renal injury. Attention must also be paid to electrolyte balance, coagulation, and the potential need for transfusion.
Hemodynamic Changes During HIPEC
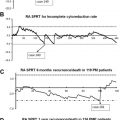
During the intraperitoneal infusion of heated chemotherapeutic agents, patients develop a hyperdynamic, vasodilated circulatory state that is characterized by steady increase in heart rate and cardiac output that reaches its maximum between 70 to 80 minutes of the 90-minute heated chemotherapy phase. As the body temperature decreases after completion of the heated therapy, the hyperdynamic state begins to normalize, but may remain above baseline 10 minutes after the chemotherapeutic lavage is concluded. When the closed abdomen technique is used, increased intra-abdominal pressure may decrease venous return, and further aggravate hemodynamic lability.
The details of these hemodynamic responses have described previously. Using esophageal Doppler to estimate cardiac output, Esquivel and colleagues documented the effect of thermal stress with subsequent development of hyperdynamic circulatory state with increased cardiac output, decreased systemic vascular resistance, increased heart rate, and increased carbon dioxide production ( Box 1 ). Although there may be a component of increased myocardial contractility, increases in cardiac output appear to be driven primarily by increased heart rate. Not surprisingly, perioperative complications may be related to acute change in body temperature and increased abdominal pressure.
- 1.
Increased cardiac output
- 2.
Decreased systemic vascular resistance
- 3.
Increased heart rate
- 4.
Increased end-tidal CO2
The use of long-acting antihypertensives is avoided because of the dynamic nature of the procedure. Heart rate is generally maintained at lower than 90 beats per minute. A cardioselective beta-blocker such as metoprolol administered in small increments provides adequate heart rate control without significant vasodilation. In accordance with recommendations by the American College of Cardiology and American Heart Association, patients on preoperative beta-blockers receive these medications perioperatively as well.
Goal-Directed Fluid Management
Although it is tempting to assume that patients undergoing HIPEC surgery will require “massive” crystalloid replacement, it is perhaps more appropriate to substitute the word “meticulous.” Fluid overload sets the stage for a variety of postoperative complications, notably pulmonary edema and adult respiratory distress syndrome. Crystalloid restriction has been demonstrated to improve outcomes after major gastrointestinal surgery. Our approach to fluid administration has gradually evolved from a traditional “cookbook” approach focused on aggressive, central venous pressure (CVP)-guided replacement of surgical “third-space” losses with crystalloids, to a more goal (flow)-directed strategy in which continuous measurement of cardiac index guides interventions, with a balance of colloids and crystalloids administered for specific therapeutic end points. A recent meta-analysis of fluid management strategies in the setting of major surgery has demonstrated the superiority of goal-directed management over liberal fluid administration in promoting good perioperative outcomes.
In addition to insensible losses (which are typically low) and hemorrhage, surgical patients may develop pathologic fluid accumulations, such as ascites and pleural effusions. Nonpathologic fluid accumulations associated with surgery are less well defined, although the concept of surgical “third spacing” is part of the conventional wisdom in both surgery and anesthesiology. The notion that tissue trauma creates a fluid-consuming third space is so basic a concept that it is presented at the introductory textbook level. Indeed, in our early management strategies for HIPEC surgery, crystalloid administration of 10 to 15 mL/kg/h was routine. The validity of the concept of third spacing, however, has been recently challenged. Experimental preparations demonstrating the existence of the third space rely on radioactive tracer methodology. A review of these studies has revealed substantial flaws in this methodology, calling into question the existence of the “third space.”
Unlike the third space, the volume-expanding effects of crystalloid solutions are well characterized. After 1 hour, only 200 mL of a 1-L crystalloid bolus remains in the intravascular space, with the remainder in the interstitium. This extravascular fluid has no volume-expanding effect, and may impair pulmonary function, and interfere with the healing of gut anastomoses. In extreme cases, perioperative weight gain secondary to crystalloids may be linked to increased mortality. Finally, it should be noted that the administration of large volumes of any type of intravenous fluids may cause dilution of platelets and coagulation factors, resulting in clinically significant coagulopathy.
Currently at our institution, continuous noninvasive cardiac output monitoring, as well as urine output, is used to guide fluid administration throughout the procedure. The noninvasive nature of this monitoring confers several advantages. Baseline stroke volume index may be obtained before the induction of anesthesia, and volume responsiveness can be established by performing a passive leg raise test (PLR). PLR causes an endogenous fluid challenge of approximately 200 mL, by moving blood normally sequestered in the calf veins into the central circulation. Patients with a 10% increase in cardiac index owing to position change are considered volume responsive. No response to PLR signifies euvolemia, or possibly depressed left ventricular function. During surgery, decreases in stroke volume index may occur because of hypovolemia, venodilation, blood loss, or decreases in venous return from mechanical causes. Fluid responsiveness is also suggested by increases in SVV. Initial therapy in this setting is generally a 500-mL colloid bolus with either 5% albumin or third-generation hydroxyethyl starch (Voluven, HES 130/0.4, Hospira, Inc, Lake Forest, IL, USA). Transfusion with packed red blood cells is rarely necessary. In our experience, typical estimated blood loss averages 300 to 500 mL.
Both human derived and synthetic colloids provide 1:1 volume-expanding effects for several hours. Voluven is favored over first-generation hydroxyethyl starches (Hespan, Hextend) for a variety of reasons. Voluven is a small molecule that is more freely filtered by the kidney, resulting in substantially less plasma and tissue accumulation, and risk of nephrotoxicity. In addition, its effect on Factor VIII and von Willebrand appear to be clinically insignificant. Patients with substantial ascites or who require extensive surgical debulking are at risk for clinically significant protein losses. Because of this, such patients may benefit from volume expansion with albumin as opposed to hydroxyethyl starch.
Renal Protection
Because some chemotherapeutic agents are nephrotoxic, maintenance of steady urine output is encouraged. Unfortunately, it is not known to what degree urine output must be maintained, and the link between intraoperative urine output and postoperative creatinine elevation is unclear. At our institution, the goal is to maintain 100 mL every 15 minutes of urine output for the duration of the hyperthermic perfusion. In some patients, urine output of 50 to 75 mL every 15 minutes may be acceptable. In addition to ensuring euvolemia with administration of both colloid and crystalloids, low-dose dopamine infusion is initiated 15 to 30 minutes before infusion of mitomycin C, and is infused only for the 90 minutes of heated perfusion. Dopamine is a nonselective DA1 and DA2 agonist with multiple dose-related effects. Although dopamine may not afford additional renal protection per se, renal perfusion may be enhanced secondary to increased cardiac output, perfusion pressure, and renal blood flow. Stimulation of DA1 receptors causes renal vasodilation as well as inhibition of active sodium transport in the proximal tubule, leading to natriuresis and dieresis, which is clinically reassuring. Furosemide should be administered only when urine output is inadequate despite confirmation of adequate intravascular volume and renal perfusion.
Temperature Management
The infusion of heated chemotherapy solution causes a gradual rise in core temperature. The temperature and urine output must be documented every 15 minutes and communicated to the surgeon and perfusionist. At some institutions, core temperature is controlled using a combination of cooling and warming regimens at the various stages of the surgery. The surgeon or perfusionist should decrease the temperature of the perfusate when the core temperature approaches 39°C. Of note, there may be disparity of temperature measurements depending on the temperature probe site. In our experience, rectal temperature may exceed nasopharyngeal temperature, possibly owing to local intraperitoneal heat transfer. Additional heat transfer to the patient should be avoided during the chemotherapy phase. At a minimum, fluid warmers must be turned off and forced air warmers should be set to ambient temperature. A strategy used in our institution is to allow patient temperature to drift to 35.5°C before the start of HIPEC.
Electrolyte Management
A variety of acid-base and electrolyte disturbances have been reported in the setting of HIPEC surgery, and may vary with the type of chemotherapeutic agents used. Oxaliplatin may predispose patients to lactic acidosis, hyperglycemia, and hyponatremia. Cisplatin may aggravate low magnesium levels, culminating in cardiac dysrhthmias. Approximately 15 minutes before the start of heated chemotherapeutic infusion, a set of laboratory studies is obtained, including chemistries, arterial blood gas, and hemoglobin. Many patients will require electrolyte replacements, most commonly calcium, magnesium, and potassium. Therefore, rechecking electrolytes after the chemotherapy phase of the procedure is prudent. In our experience, the development of acidosis is rare, particularly if adequate cardiac output is maintained. A checklist provides a useful strategy for ensuring that key tasks are accomplished before starting HIPEC ( Box 2 ).
Related posts:
 The Importance of the Learning Curve and Surveillance of Surgical Performance in Peritoneal Surface Malignancy Programs
The Importance of the Learning Curve and Surveillance of Surgical Performance in Peritoneal Surface Malignancy Programs
 Current Status and Future Directions in Appendiceal Cancer with Peritoneal Dissemination
Current Status and Future Directions in Appendiceal Cancer with Peritoneal Dissemination
 Pharmacology of Perioperative Intraperitoneal and Intravenous Chemotherapy in Patients with Peritoneal Surface Malignancy
Pharmacology of Perioperative Intraperitoneal and Intravenous Chemotherapy in Patients with Peritoneal Surface Malignancy
 Early Intervention for Treatment and Prevention of Colorectal Carcinomatosis
Current Status and Future Directions of Cytoreductive Surgery and Hyperthermic Intraperitoneal Chemotherapy in the Treatment of Ovarian Cancer
Early Intervention for Treatment and Prevention of Colorectal Carcinomatosis
Current Status and Future Directions of Cytoreductive Surgery and Hyperthermic Intraperitoneal Chemotherapy in the Treatment of Ovarian Cancer
 Randomized Clinical Trials for Colorectal Cancer Peritoneal Surface Malignancy
Randomized Clinical Trials for Colorectal Cancer Peritoneal Surface Malignancy
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


