Anatomy and Physiology Applied to Infusion Therapy
Anatomy and Physiology Applied to Infusion Therapy
Sharon M. Weinstein
KEY TERMS
Aberrant Artery
Afferent
Arterial Spasm
Arteriovenous Anastomosis
Autonomic Nervous System
Clotting Cascade
Efferent
Extrapyramidal Side Effects
Integument
Somatic Nervous System
Superficial Fascia
Tunica
Valves
Vascular System
Vasovagal Reaction
Velocity
VASCULAR ANATOMY AND THERAPEUTIC GOALS
Because infusion therapy involves the administration of fluids, blood, and drugs directly into the vascular system—that is, into arteries, bone marrow, and veins—the nurse and others responsible for administering therapy need to understand the anatomy and physiology of vascular structures and related systems.
Knowing the functions of the cardiovascular system and the parts of the body that are part of it is critical in understanding the physiology of the human body. With its complex pathways of veins, arteries, and capillaries, the cardiovascular system keeps life pumping through you. The heart, blood vessels, and blood help to transport vital nutrients throughout the body as well as remove metabolic waste. They also help to protect the body and regulate body temperature.
Although the veins, because of their abundance and location, provide the most readily accessible route for infusion therapies, the arteries and bone marrow are also used. Arteries provide the route for introducing radiopaque material for diagnostic purposes, such as in arteriograms to detect cerebral disorders; blood pressure monitoring, determinations of arterial blood gas levels, and administration of chemotherapy. The dangers of arterial spasm and subsequent gangrene present problems that make this route of therapy hazardous for therapeutic use. The bone marrow, because of its venous plexus, is used for infusion therapy by the intraosseous route.
The primary goal of infusion (IV) therapy is to provide a positive outcome for the patient. Painless and effective therapy is desirable, promoting the patient’s comfort, wellbeing, and often complete recovery from disease or trauma. An integral part of this goal is the recognition and prevention of complications. To achieve the goal and minimize the risk of complications, the IV nurse needs a solid knowledge of vascular anatomy and physiology.
PATIENT SAFETY
The primary goal is to ensure a safe outcome for the patient.
Integration of Knowledge with Practice
By studying the superficial veins, the nurse learns to discriminate the most appropriate veins to use for infusion therapy. Factors to be considered in selecting a vein include size, location, and resilience. In addition, understanding the reaction of veins to the nervous stimulation of the vasoconstrictors and vasodilators enables the clinician to increase the size and visibility of a vein before attempting venipuncture and to relieve venous spasm and thus assist in infusion maintenance.
By studying the superficial veins of the lower extremities, the nurse becomes alert to the dangers resulting from their use. Avoiding venipuncture in veins susceptible to varicosities and sluggish circulation decreases the likelihood of complications, such as phlebitis and thrombosis, and reduces the secondary risk of pulmonary embolism.
Common Venous Complications
Phlebitis and thrombosis are by far the most common complications resulting from parenteral therapy. Although seemingly mild, phlebitis and thrombosis may have serious consequences. First, they cause moderate to severe discomfort, often taking many days or weeks to subside. Second, they limit the veins available for future therapy. Injury to the endothelial lining of the vein contributes to these local complications.
Crucial to recognizing and preventing complications is a solid knowledge of the characteristics that differentiate veins from arteries and the positions of each. Understanding this helps the nurse avoid the complications of an inadvertent arterial puncture. The knowledge also helps to reduce the risk of necrosis and gangrene and to recognize the existence of an arteriovenous anastomosis, a congenital or traumatic abnormality in which blood flows directly from the artery into the vein.
Failure to recognize an arteriovenous anastomosis results in repeated and unsuccessful venipunctures performed in an attempt to initiate the infusion. Repeated punctures compound the trauma to the inner lining of the vein and increase the risk of the local complications already described, any one of which limits the number of available veins, interrupts the course of therapy, and causes unnecessary pain or, possibly, dire consequences for the patient.
SYSTEMS AND ORGANS INVOLVED IN INFUSION THERAPY
Among the organs and systems closely associated with infusion therapy are the integumentary, neurologic, cardiovascular, and respiratory systems, as well as individual circulatory organs and structures.
Integument and Connective Tissue
The integument, or skin, is the first organ affected in IV access. It protects the body from the environment and is a natural barrier to external forces. It ranges in thickness from 1.5 to 4.0 mm, with the thickest skin appearing on the palms of the hands and plantar aspect of the feet. The skin also synthesizes vitamin D, cytokines, and other growth factors; is influenced by hormones; and assists in the control of body temperature (Standring, 2008). The skin is made up of two layers, the epidermis and the dermis. See Table 6-1: Layers of the epidermis.
EPIDERMIS
The epidermis is the uppermost layer, which forms a protective covering for the dermis. Its thickness varies in different parts of the body and is thickest on the palms of the hands and the soles of the feet and thinnest on the inner surface of the limbs. Thickness is a variable of the aging process and medications such as prednisone. In an elderly patient, for example, the skin on the dorsum of the hand may be so thin that it does not adequately support the vein for venipuncture when parenteral infusions are required.
TABLE 6-1 LAYERS OF THE EPIDERMIS
Layer
Characteristics
Stratum corneum
Many layers of dead, anucleate keratinocytes completely filled with keratin
The outermost layers are constantly shed.
Stratum lucidum
Two to three layers of anucleate cells
This layer is found only in “thick skin” such as the palm of the hand and the sole of the foot.
Stratum granulosum
Two to four layers of cells held together by desmosomes
These cells contain keratohyalin granules, which contribute to the formation of keratin in the upper layers of the epidermis.
Stratum spinosum
Eight to 10 layers of cells connected by desmosomes
These cells are moderately active in mitosis.
Stratum basale
Single layer of columnar cells actively dividing by mitosis to produce cells that migrate into the upper epidermal layers and ultimately to the surface of the skin
Adapted from CliffsNotes.com. The epidermis. (2013). http://www.cliffsnotes.com/study_guide/The-Epidermis.topicArticleId-277792,articleId-277538.html
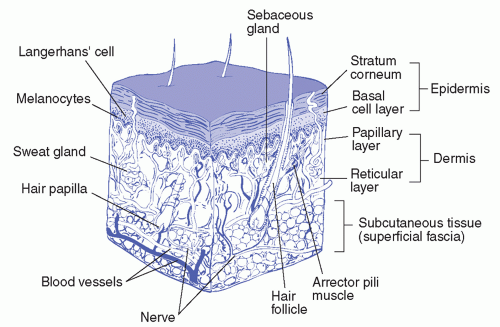
FIGURE 6-1 Layers of the skin. The epidermis protects the highly vascular dermis that lies above the superficial fascia (subcutaneous tissue).
DERMIS
The dermis, or underlayer, is highly sensitive and vascular. It contains many capillaries and thousands of nerve fibers (Figure 6-1). See Table 6-2: Layers of the Dermis.
SUPERFICIAL FASCIA OR HYPODERMIS
The superficial fascia, or subcutaneous areolar connective tissue, lies below the two layers of skin and is, itself, another covering. The superficial veins are located in this fascia, which varies in thickness. When a catheter is inserted into this fascia, there is free movement of the skin above. Great care and meticulous aseptic technique must be observed because an infection in this loose tissue spreads easily. Such an infection is called cellulitis (Williams, Warwick, Dyson, & Bannister, 1995).
TABLE 6-2 LAYERS OF THE DERMIS
Layer
Characteristics
Papillary
Thin outer layer of areolar connective tissue with fingerlike projections called dermal papillae that protrude into the epidermis
Reticular
Thick layer of dense irregular connective tissue, which lies deep to the papillary layer and makes up most of the dermis
Adapted from CliffsNotes.com. The dermis. (2013). http://www.cliffsnotes.com/study_guide/The-Dermis.topicArticleId-277792,articleId-277540.html
Neurologic System
The human nervous system is an integral loop containing billions of neurons and hundreds of thousands of synaptic connections. Changes in the environment trigger a response by the main controlling organ, the brain, which coordinates and processes the information, determines a response mechanism, and then communicates that response back to the body.
FUNCTIONAL
SENSORY RECEPTORS
A characteristic of a living organism is its ability to respond to stimuli. The human sensory system is highly evolved and processes thousands of incoming messages simultaneously. This complexity allows you to be aware of your surroundings and take appropriate actions. They are classified by type, location, and type of stimulus detected. For example,
Mechanoreceptors respond to physical force such as pressure (touch or blood pressure) and stretch.
Photoreceptors respond to light.
Thermoreceptors respond to temperature changes.
Chemoreceptors respond to dissolved chemicals during sensations of taste and smell and to changes in internal body chemistry such as variations of O2, CO2, or H+ in the blood.
Nociceptors respond to a variety of stimuli associated with tissue damage. The brain interprets the pain (CliffsNotes, 2013).
MOTOR FUNCTION
Sensory information is transmitted from all areas of the nervous system into the spinal cord, brain stem, and cerebrum where it produces muscular functions transmitted to the body along efferent nerve fibers. The term extrapyramidal side effect is sometimes used to describe involuntary motor movements of the neck, jaw, and extremities with the administration of some types of medications (Hadaway, 2010).
ANATOMICAL
CENTRAL NERVOUS SYSTEM
The central nervous system (CNS) consists of the brain and spinal cord. The spinal cord extends from the medulla oblongata and occupies approximately two thirds of the length of vertebral column. The cord is enclosed within three protective layers: the pia mater, the arachnoid mater, and the dura mater, which is most distal.
PERIPHERAL NERVOUS SYSTEM
The peripheral nervous system (PNS) consists of nerves outside the CNS. Nerves of the PNS are classified in one of two ways: first, by how they are connected to the CNS. Cranial nerves originate from or terminate in the brain, while spinal nerves originate from or terminate at the spinal cord and then by the direction of nerve propagation. Sensory (afferent) neurons transmit impulses from the skin and other sensory organs or from various places within the body to the CNS. Motor (efferent) neurons transmit impulses from the CNS to effectors (muscles or glands). Secondly, motor neurons are further classified according to the effectors they target or function. The somatic nervous system (SNS) directs the contraction of skeletal muscles. The autonomic nervous system (ANS) controls the activities of organs, glands, and various involuntary muscles, such as cardiac and smooth muscles.
The ANS is further divided in two:
The sympathetic nervous system is involved in the stimulation of activities that prepare the body for action, such as increasing the heart rate, increasing the release of sugar from the liver into the blood, and other activities generally considered as fight or flight responses.
The parasympathetic nervous system activates tranquil functions, such as stimulating the secretion of saliva or digestive enzymes into the stomach and small intestine.
Both sympathetic and parasympathetic systems target the same organs but often work antagonistically. For example, the sympathetic system accelerates the heartbeat, while the parasympathetic system slows the heartbeat. Each system is stimulated as is appropriate to maintain homeostasis.
The nervous system responds to changes in the environment through sensory organs and is responsible for
Sensory function, transmitting information from tactile, visual, and auditory receptors
Motor functions, controlling skeletal and smooth muscle
Autonomic function, controlling glands and smooth muscle
Nerve fibers under the skin include those that react to temperature, touch, pressure, and pain. The number of nerve fibers varies in different areas of the body. Some areas of the skin are highly sensitive; other areas are only mildly sensitive. The insertion of a needle in one area may cause a great deal of pain, yet another area may be virtually insensitive to pain. The inner aspect of the wrist is a highly sensitive area. Venipunctures are performed here only when other veins have been exhausted.
The anatomic divisions of the nervous system are the CNS (the brain and spinal cord) and PNS (12 cranial and 31 spinal nerves). The vagus nerve, which innervates the heart, is of prime importance. Stimulation of the vagus nerve produces a depressant effect on cardiac muscle, resulting in clinical signs such as bradycardia and hypotension. This condition is known as a vasovagal reaction or vasovagal syncope.
Cardiovascular System
The blood volume and distribution, for which the circulatory system is responsible, result from complex interactions among cardiac output, excretion of fluids and electrolytes by the kidneys, and hormonal and nervous system factors. Total blood volume may be enhanced by pregnancy, large varicose veins, polycythemia, and inability of the heart to pump enough blood to perfuse the kidneys.
Only gold members can continue reading. Log In or Register to continue
 PATIENT SAFETY
PATIENT SAFETY