Alcohol
Alcoholism
Alcohol intoxication
Alcohol treatment
Alcohol use
Binge drinking
Screening and brief intervention
Underage drinking
Incidence: 18.6% of high school youth in the US reported that they drank alcohol before the age of 13 years (for the first time, other than a few sips).
Lifetime prevalence: 66.2% reported that they ever had at least one drink of alcohol (on at least one day during their life).
Current prevalence: 34.9% reported that they currently drank alcohol (had at least one drink of alcohol on at least 1 day during the past 30 days).
Binge drinking: Binge drinking is defined as excessive alcohol intake within a 2-hour period such that BAC levels reach 0.08 g/dL (the legal limit of intoxication) or more. This typically happens when males consume five drinks or more and when women drink four drinks or more, within a 2-hour period.1 Research suggests that for 9- to 13-year-old children and girls aged 14 to 17 years, binge drinking should be defined as three or more drinks. For boys, binge drinking should be defined as four drinks or more for those aged 14 or 15 years and five or more drinks for those aged 16 or 17 years. These figures are based on the number of drinks required to reach a BAC of 0.08 g/dL.1 Data suggest that 20.8% of adolescents reported that they had five or more drinks of alcohol in a row (within a couple of hours on at least 1 day in the past month).
Monitoring The Future (MTF): Data from the 2014 MTF survey reveal lifetime, current, and binge drinking trends across 8th, 10th, and 12th grade levels3:
Lifetime prevalence: The prevalence of lifetime alcohol use for 8th, 10th, and 12th graders combined in 2014 was 40.7%. The percentage reporting ever being drunk in one’s lifetime across all three grade levels was 23.6%.
Current prevalence: Current alcohol use (drinking in the 30-day period prior to the survey) was 9% for 8th graders, 24% for 10th graders, and 37% for 12th graders. Overall, the current prevalence in the past month across the three grades combined in 2014 was 22.6%.
Binge drinking: The proportion of binge drinking (i.e., having five or more drinks in a row at least once in the prior 2 weeks) for 8th, 10th, and 12th graders was 5.1%, 13.7%, and 22.1%, respectively. Overall, the current prevalence of binge drinking during the past month across the three grades combined was 11.7%.
National Survey on Drug Use and Health (NSDUH): Data from the NSDUH (2014) survey also provide current, binge, and heavy alcohol use among adolescents in the US.4 The NSDUH defines current (past month) use as at least one drink in the past 30 days; binge use as five or more drinks on the same occasion (i.e., at the same time or within a couple of hours of
each other) on at least 1 day in the past 30 days; and heavy use as five or more drinks on the same occasion on each of 5 or more days in the past 30 days:
TABLE 64.1 Effects of Alcohol Consumption in the Nontolerant Individual
Blood Alcohol Level (g/dL)
Effects
0.02
Reached after approximately one drink; light or moderate drinkers feel some effect—warmth and relaxation
0.04
Most people feel relaxed, talkative, and happy; skin may become flushed
0.05
First sizable changes begin to occur; light-headedness, giddiness, lowered inhibitions, and less control of thoughts may be experienced; both restraint and judgment are lowered; coordination may be slightly altered
0.06
Judgment is somewhat impaired; ability to make rational decisions about personal capabilities is affected (such as being able to drive)
0.08
Definite impairment of muscle coordination and slower reaction time occurs; driving ability becomes suspect; sensory feelings of numbness of the cheeks and lips occur; hands, arms, and legs may tingle and then feel numb (this constitutes legal impairment in Canada and in some US states, e.g., California)
0.10
Clumsiness; speech may become fuzzy; clear deterioration of reaction time and muscle control (this level previously constituted drunkenness in most US states)
0.15
Definite impairment of balance and movement
0.20
Motor and emotional control centers are measurably affected; slurred speech, staggering, loss of balance, and double vision can all be present
0.30
Lack of understanding of what is seen or heard occurs; individuals are confused or stuporous and may lose consciousness
0.40
Usually unconscious; the skin becomes clammy
0.45
Respiration slows and may stop altogether
0.50
Death occurs
From Morrison SF, Rogers PD, Thomas MH. Alcohol and adolescents. Pediatr Clin North Am 1995;42:371-387.
Current use: Of the approximately 24.3 million adolescents in the US, 16.6% had used alcohol in the past month (10.3% to the point of intoxication), with 8.0% meeting criteria for substance abuse/dependence in the past year.3 Data also show that rates of current alcohol use were lowest for youth aged 12 or 13 (2.1%) and increased with age (9.5% for 14- to 15-year-olds and 22.7% for 16- to 17-year-olds).
Binge drinking: Rates of binge alcohol use followed trends similar to current use, with rates lowest for 12- to 13-year-olds (0.8%) and increasing to 4.5% for 14- to 15-year-olds and 13.1% for 16- to 17-year-olds.
Heavy drinking: Heavy alcohol use rates for adolescents aged 12 to 13 and 14 to 15 were less than 1% (0.1% and 0.7%, respectively) and up to 3% for 16- to 17-year-olds.
Lifetime prevalence: Lifetime prevalence of alcohol use for young adults in 2014 increased with age: 72.1% for 19- to 20-year-olds; 85.2% for 21- to 22-year-olds; 88.8% for 23- to 24-year-olds; and 91.1% for 25- to 26-year-olds.
Annual prevalence: The annual prevalence of alcohol use for young adults followed a pattern comparable to those of lifetime rates in 2014: 68.4% for 19- to 20-year-olds; 82.8% for 21- to 22-year-olds; 84.7% for 23- to 24-year-olds; and 87.9% for 25- to 26-year-olds.
Current use: The current rates of alcohol use (past 30 day use) for young adults also escalated with increasing age: 51.5% for 19- to 20-year-olds; 70.5% for 21- to 22-year-olds; 72.7% for 23- to 24-year-olds; and 75.9% for 25- to 26-year-olds.
Binge drinking: The proportion of young adults who reported binge drinking (i.e., having five or more drinks in a row at least once in the prior 2 weeks) was lower for 19- to 20-year-olds (27.2%) compared to 21- to 22-year-olds, 23- to 24-year-olds, and 25 to 26-year-olds (40%, 38%, and 37%, respectively).
Current use: Rate of current alcohol use in 2013 among young adults aged 18 to 25 was 59.6%.
Binge drinking: Rates of binge drinking among young adults ranged from 29.1% among 18- to 20-year-olds to 43.3% for those aged 21 to 25. Figure 64.1 shows that young adults aged 18 to 25 have the highest prevalence of binge drinking in the US (estimated at 37.9%).
Heavy drinking: Rates of heavy alcohol use in 2013 were 8.5% for young adults aged 18 to 20, peaking at 13.1% for those aged 21 to 25. As a whole, heavy alcohol use was reported by 11.3% of young adults aged 18 to 25 years.
According to 2013 data from the American College Health Association’s National College Health Assessment (NCHA) survey,6 the proportion of young adult college students who reported any alcohol use within the last 30 days was 66.8% (67.0% for females and 66.8% for males).
with the exception of the 19- to 22-year-old age-group. Specifically, males in this age-group have higher rates of daily drinking than their female age counterparts (5.6% for males versus 2.4% for females).
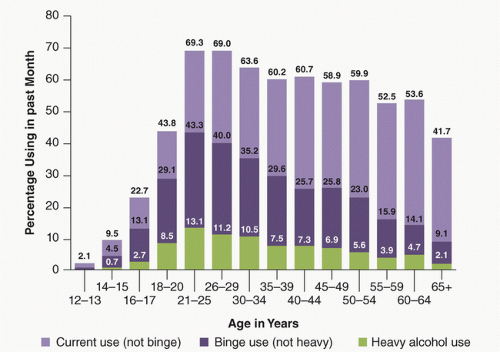 FIGURE 64.1 Percentage of current, binge, and heavy drinking by age-groups in the US. Results from the 2013 National Survey on Drug Use and Health: Summary and National Findings. |
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


