Mishaps are like knives, that either serve us or cut us, as we grasp them by the blade or the handle.
—James Russell Lowell
We shall draw from the heart of suffering itself the means of inspiration and survival.
—Winston Churchill
There has been a massive increase in the online community with a commensurate increase in the ability of Internet-based searches to find and retrieve safety information. Aviation safety databases maintained by individuals and government agencies have increased in scope and content. A public aeromedical mailing list, published by an Internet list server instantly from reader postings, has existed for more than a decade and knits together aeromedical practitioners the world over. The safety statistics and research findings presented here are available from various government, industry, academic, and aviation advocate organizations through their various websites, so the reader will be able to acquire the most up-to-date information to complement the information presented in this chapter. The National Transportation Safety Board (NTSB) investigation and studies, the Air Accidents Investigation Branch, the General Aviation Manufacturers Association data, the Flight Safety Foundation, the National Business Aircraft Association, the Aircraft Owners and Pilots Association (AOPA) safety database, the Federal Aviation Administration (FAA) Aviation Safety Data, and the Civil Aerospace Medical Institute (CAMI) publications are all available online. These websites and more are easily retrieved by entering in the search terms “aviation safety” or the title of the organization in a search engine. Many governments have committed to making much of its safety data available online to provide a comprehensive, convenient, and low-cost access to nonprivacy materials. The development of powerful, comprehensive, and logical Internet search engines will allow the reader to continue to find such safety data even as the Internet addresses of the various entities may change over time. Some useful universal resource locators (URLs) will be included in the text and some are appended at the end of this chapter to find these various information resources. In addition, the number of agencies that have become involved with the aircraft accident disaster scene has increased, resulting in increased complexity in managing an aircraft accident investigation. Although the safety statistics may change over time to reflect an improvement in aerospace safety, and technology continues to add more sophisticated accident reconstruction tools, many of the original investigative techniques for medical aircraft accident investigation are sound and will serve the aerospace medicine practitioner well in their participation in aircraft accident investigations.
PURPOSE OF THE INVESTIGATION
There are many reasons to investigate aerospace accidents and incidents. Primarily there is the need to prevent future occurrences. Of secondary importance is the need to learn about the failure modes of people, equipment, and systems in aerospace. A sudden occurrence of a mass disaster, such as an aircraft accident, with the attendant instant media coverage around the world, arouses public concern. After the accident, affected individuals and organizations will have substantial personal interests in the findings and determinations of accident investigations. Survivors of those who die in the crash are interested in obtaining adequate explanation as they try to come to terms with the loss of loved ones. The local government has an interest in ensuring the health, safety, and welfare of the public. It wants to be sure that no crime against the state or individuals has been committed and that there is no risk of infectious disease. The local jurisdiction is responsible for determining the manner of death of the accident victims and to properly handle the human remains. Environmental damage and hazardous materials caused by the accident bring other federal agencies into the investigation and cleanup efforts. The federal government has many of the same interests as the local government. In addition, it is also concerned with the safe and efficient operation of interstate commerce. There will always be substantial legal proceedings occurring in background of investigations and this should not deter the medical accident investigator from their tasks. The recent development of commercial space flight will further necessitate the development of resources to properly investigate space-based accidents.
Investigators feel the pressure of all these interests, but they must not forget that the primary purpose of aircraft accident investigation is to prevent future accidents, injuries, and fatalities. To achieve this goal, they must thoroughly investigate all injuries and circumstances of a mishap, avoiding the placing of blame and seeking the root causes of the accident. They must concentrate on the most proximal of events in the complex sequence of linked events that always precede the accident occurrence, and must look for all factors that may have contributed to the accident. They must also avoid premature analyses and conclusions by keeping an open mind and concentrating on collecting facts during the investigation.
ROLE OF THE PHYSICIAN IN AIRCRAFT ACCIDENT PREVENTION
This chapter provides useful information for all who participate in accident investigation and prevention activities. There are many types of individuals from many disciplines that comprise the modern group-based investigation of the medical aspects of accidents. In this group, one will find anthropologists, pilots, flight attendants, air traffic specialists, psychologists, physiologists, coroners and medical examiners, safety engineers, and aerospace medicine practitioners. The primary role of the aerospace medicine practitioner in aerospace accident investigation is to examine both the causes and consequences of the accident, in order to learn how to prevent the occurrence. A secondary role is to document from the consequences of the accident how to improve survivability and to reduce deaths and injuries that occur when the accident is not prevented.
There are additional means by which military flight surgeons, aviation medical officers, and designated aviation medical examiners (DAME) participate in preventing aircraft accidents. As medical practitioners, they have a role in certifying their pilot patients fit for flight. Some practitioners develop comprehensive preventive medicine programs for their pilots. In most countries, a physician is making a finding, under the regulations of those countries, that the pilot is not likely to sustain an incapacitation during the period of the validity of the certification, which may span time intervals of several months to several years. In the case of multicrew cockpit operations the certification that a particular pilot is fit, in other words that the pilot will not have an in-flight incapacitation, is important. In single-pilot cockpit operations, it is potentially a life-or-death decision because the certified pilot may be the only person able to fly the aircraft. Therefore if they are incapacitated there is almost a certainty of a crash.
There is a potential conflict in treating pilots and always maintaining their confidentiality. In some cases, aviation safety problems are prevented when treating physicians (or other health care professionals) after providing medical care, also forward information regarding the pilot’s medical condition to aviation authorities. Some jurisdictions, like Canada, require the reporting to the federal civil aviation authorities of serious medical conditions in pilots that may pose aviation safety risks, and require that aircrew members identify themselves as aircrew to health care providers. DAMEs can serve as the pilot’s best advocate to maintain medical certification of fitness to fly. However, accidents have occurred when pilots hid known medical conditions, and when some physicians participate in the misdirected actions of protecting or assisting the pilot in concealing medical conditions. A fatal accident occurred when a pilot became incapacitated and the investigation uncovered the deceit of the airmen and his aviation medical examiner (AME) in concealing cardiac disease (NTSB Case Number: CHI02FA172). Investigation of medically related accidents and incidents can also serve as a quality control function for medical certification authorities by providing long-term data to assist in evidence-driven medical certification decision making.
DEFINITIONS OF INCIDENT, ACCIDENT, AND FATALITY
The NTSB defines accident as “an occurrence associated with the operation of an aircraft which takes place between the time any person boards the aircraft with the intention of flight until such time as all such persons have disembarked, in which any person suffers death or serious injury as a result of being in or upon the aircraft or by direct contact with the aircraft or anything attached thereto, or the aircraft receives substantial damage. Fatal injury means any injury which results in death within 30 days of the accident. Incident means an occurrence other than an accident, associated with the operation of an aircraft, which affects or could affect the safety of operations” (1).
It is important to understand the background of cultural and historical perceptions of accidents. In the history of crash investigation, famous researchers showed that aviation accidents were not inevitable acts of nature or unpreventable occurrences. Highlighting this cultural misperception, dictionary definitions of accident have many clauses and interpretations. One of the most comprehensive definitions of accident can be found in the 1999 edition of the Microsoft (MS) Encarta World English Dictionary, partly excerpted here, accident* is defined as follows (2):
1) Chance: the way things happen without any planning, apparent cause, or deliberate intent; 2) Crash: a collision or similar incident involving a moving vehicle, often resulting in injury or death; 3) Mishap: an unplanned and unfortunate event that results in damage, injury, or upset of some kind; and 4) Chance happening: an event that happens completely by chance, with no planning or deliberate intent.
None of these definitions convey the proper sense that accidents can be prevented. The legal NTSB definition will be given later. Although accident is a commonly accepted term, many of the aerospace occurrences that are called accidents are not unforeseen, and some, to the aviation safety expert, are predictable in that they have readily apparent causes. The occurrences of deliberate destructive acts, such as suicide or sabotage, are not included in safety data rates by the NTSB, the FAA, or the industry. Accidents resulting from suicide and sabotage are not addressed in this chapter, although there have been useful studies of the use of aircraft as instruments of self-destruction. U.S. military forces use the term mishap rather than accident. Some researchers advocate the term crash, but not all accidents or incidents involve a crash event. Since 1995, coordinated by the Joint Committee on Aviation Policy, accidents involving public use aircraft have been investigated by the affected government agency, using NTSB standards or staff participation, and have been reported to the NTSB. They are not discussed here.
SAFETY STATISTICS
With the United States incurring much of the world’s aviation activity, and carrying slightly less than half the world’s airline passengers, there is a wealth of data in the National Airspace System (NAS). The FAA is responsible for monitoring and managing the NAS and all safety measures and is establishing an Aviation Safety Information Analysis and Sharing System (http://www.faa.gov/safety/). Online data searches can be made of aviation incidents from the FAA investigations, and aviation accidents, from NTSB investigations. The NTSB also makes its investigation records available to online query and the datasets can be downloaded in their entirety (www.ntsb.gov).
The NAS Information Monitoring System [National Airspace System Information Monitoring System (NAIMS)] produces the Aviation Safety Statistical Handbook (3). As of April 2007, this handbook contains 5 years of data, with accident rates for large air carriers, commuter air carriers, air taxis, general aviation, rotorcraft, and midair collisions. Five years of incident rates for air carriers, commuter air carriers, air taxis, general aviation, and rotorcraft are also provided. The NAIMS segments monitored comprise “Near Midair Collisions,” “Operational Errors,” “Operational Deviations,” “Pilot Deviations,” “Vehicle/Pedestrian Deviations,” “Surface Incidents,” “Runway Incursions,” “Flight Assists,” and NTSB accident data. In addition to the safety data and charts, contact information, an acronym/abbreviation list, and a glossary are provided. There are numerous other data products, such as the Administrators Fact Book and links to other safety datasets, such as the Bureau of Transportation Statistics, that can be found at the website listed previously.
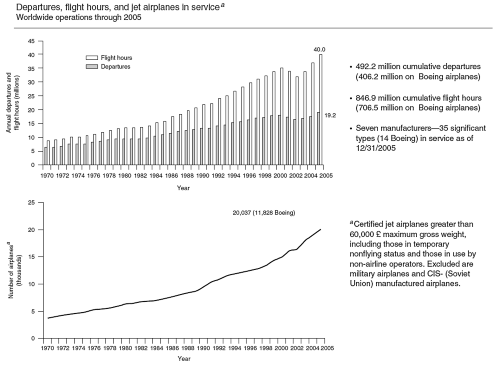
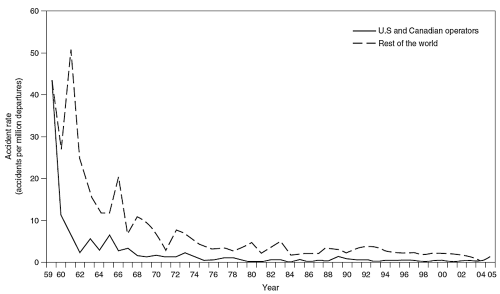
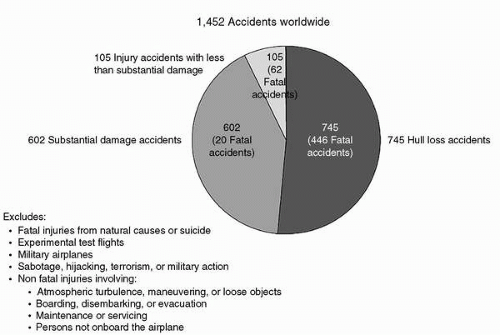
The FAA Office of System Safety originally sponsored a worldwide project called Global Aviation Information Network (GAIN), whose purpose is to develop a variety of safety measures that can be collected and shared worldwide. This sponsorship ended in 2007. The Flight Safety Foundation now maintains many of the products that were developed in GAIN. The Boeing aircraft industry company tracks safety data worldwide for large jet aircraft, regardless of manufacturer, and produces an annual summary that can be downloaded in portable document format from their website (Statistical Summary of Commercial Jet Airplane Accidents: Worldwide Operations 1959-2005, published May 2006). The number of jet aircraft worldwide has steadily increased to 20,037, and the number of commercial departures and flight hours has grown to 40.0 million and 19.2 million, respectively (Figure 25-1). These data clearly show a remarkable decrease in the worldwide accident rate, but this rate has leveled off and has remained relatively stable over the last two decades (Figure 25-2). Worldwide summary data of accidents by damage and injury is illustrated in Figure 25-3. An NTSB study of airline safety revealed that passenger enplanements in the United States more than doubled in the 16 years following 1983 (4). According to FAA data, there were 741 million domestic passenger enplanements in the United States in 1996 (not including international passenger traffic) and 2.2 billion worldwide according to International Civil Aviation Organization (ICAO) data. According to recent FAA forecasts, this growth is expected to continue, approaching 1 billion enplanements by 2015. Despite the growing demands on the U.S. aviation system, the system continues to maintain its high level of safety. The accident rate for commercial aircraft has remained approximately the same for the last two decades. If the accident rate continues, however, increased traffic projected over the next 10 years will be accompanied by a commensurate increase in the number of aircraft accidents. To prevent this from occurring, government agencies are working with industry to reduce the accident rate and number of fatalities. There are two ways to prevent fatalities in air travel: by preventing accidents and by protecting aircraft occupants in the accidents that do occur. A reduction in accident rates provides an indication of the success of accident prevention; examining occupant survivability can indicate the positive results from occupant protection. Examining occupant survivability in aviation accidents can help dispel a public perception that most air carrier accidents are not survivable, and can identify factors that can be acted upon to increase survivability in the accidents that do occur. The aerospace medicine practitioner has an important role in a multidisciplinary effort to examine both aeromedical and human factor inputs into accident causation. Aerospace medicine practitioners are ideal assets in determining the consequences of the accidents by learning how to practice primary prevention of the occurrence and documenting data from the consequences of the accident to learn how to improve secondary prevention of the deaths and injuries that result post impact. There is also much to be learned from studying the survival factors in the postimpact environment, such as factors that affect the crews’ ability to conduct the emergency egress, and the passengers’ success or failure in evacuating the aircraft.
FIGURE 25-1 Worldwide jet operations from 1970 through 2005 illustrating the number of aircraft accidents, deaths, and death rate per 100 million passenger miles (Boeing safety data, May 2006).
Safety Perspective
To understand how low aviation fatalities are related to the overall transportation safety record, and with accidents in general, it is appropriate to point out that passenger transportation accidents of all modes account for approximately one fourth of all accidental deaths. Of all types of transportation, only transit buses have a lower death rate than scheduled airliners (Table 25-1).
Later in this chapter the various types of aviation operations will be compared. A perspective of various types of risk can be made using data from the Department of Transportation (DOT) Office of Hazardous Materials Safety. This office publishes a Risk Comparison, which contains a variety of activities, including natural phenomenon, and the risk of accidental death in the United States for the period 1999 to 2003 (Table 25-2) (http://hazmat.dot.gov/riskmgmt/riskcompare.htm).
For Part 121 and 135 air carriers, with a 5-year average of 138 deaths, they calculate a general population risk of death per year of 1 out of 2,067,000, and an exposure risk of 1.9 deaths per 100 million aircraft miles.
FIGURE 25-2 Worldwide jet accident rates 1959 to 2005 for U.S. and Canadian operators compared with the rest of the world (Boeing safety data, May 2006).
FIGURE 25-3 Accident summary by damage and injury, 1959 to 2005 (Boeing safety data, May 2006).
TABLE 25-1
National Transportation Safety Board 2004-2005 U.S. Transportation Fatalities
cIncludes vehicle occupant fatalities in other vehicle types, for example, farm or construction equipment.
dGrade crossing fatalities are not counted as a separate category for determining the grand totals because they are included in the highway and rail categories, as appropriate.
eData reported to Federal Rail Administration FRA.
fIncludes persons on railroad property with and without permission. Does not include motor vehicle occupants killed at grade crossings.
gData reported to the FTA. Fatalities for commuter rail operations may also be reported to the FRA and may be included in the intercity railroad fatalities.
iIncludes non-U.S. registered aircraft involved in accidents in the United States.
Accident rates for all types of operations are available from the FAA, NTSB, and the Bureau of Transportation Statistics websites but are usually 1 to 2 years out of date. The most recent data are usually preliminary and subject to change. A variety of exposure measurements are used in the transportation industry, including time, distance, passengerdistance product, and takeoffs and landings. There is no consensus regarding common denominators of exposure, but the most often quoted rates employ 100,000 hours of flight time or 100,000 departures. Depending on the choice of an exposure denominator for risk calculations, one can get varying results. Some estimates of flying hours are indirect, using a proxy such as fuel receipts, surveys of fixed base operators or, are more direct with the use of a voluntary pilot survey. There is a great deal of variation in these methods and some recent government attempts have been launched to obtain a better measurement of these needed indices that will be of particular importance in general aviation operation estimates. Even in the presence of better exposure data it is important to consider the choice of the measurement method because the perception of the level of safety of any given aviation operation can be made to vary as different methods are employed. To be able to evaluate the effect of changes in the aviation regulatory environment, one must consider carefully the analytic methods that will perform the best in visualizing the effect of the changes. As an example of a useful statistical analysis there is a technique called segmented linear regression to examine trend data of active pilots. In one paper in 1988, several risk metrics were examined graphically, critiqued, and compared. The risk metrics examined included:
Fatalities per hour of exposure to air transportation
Passenger fatalities per 100 million scheduled passenger miles
Fatal accidents per 100,000 flights
Probability of being killed in an air carrier accident
Total accidents per 10 million system flying hours
Miles flown between successive accidents and
Mean time between failures
The paper concludes that there is no unique or correct way of measuring risk in air transportation, and that risk studies should state the applicability, spectrum, and limitations of the chosen risk metrics (5).
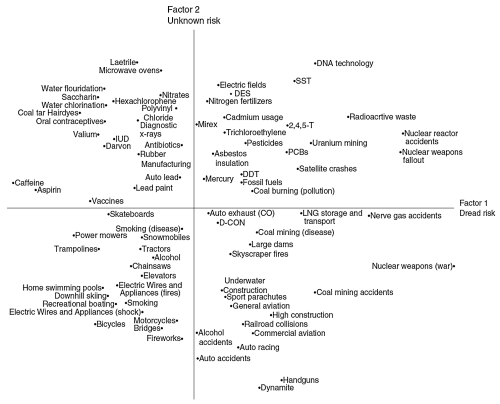
An interesting visualization for the purposes of communicating risk perspectives was published in Scientific American in July 2003 from the work of Slovic, Weber (2002) which was itself based on a publication by Slovic in Science in 1987 (http://www.ldeo.columbia.edu/chrr/documents/meetings/roundtable/white_papers/slovic_wp.pdf).
Figure 25-4 shows a risk space in two dimensions, with a vertical axis of the perception of how observable, or known the risk is, and a horizontal axis that depicts the perception of how controllable or dangerous the perceived consequences of the event are. General aviation and commercial aviation are in the lower right quadrant of the graph that was the result of his study of the public perception of risk. Note that in his graph the public perception of aviation is quite dangerous and uncontrollable considering the other activities shown close to the aviation markers. The association of aviation in an area of known, observable, but somewhat uncontrollable area of risk can be contrasted with the objective data that has been collected from many years of accident investigation and prevention.
TABLE 25-2
Risk Comparison from the Department of Transportation (DOT) Office of Hazardous Materials Safety. A Comparison of Risk Accidental Deaths—United States—1999-2003
aAn average of approximately 285,000,000 over the period was used in computations.
bTraffic Safety Facts 2004, Department of Transportation’s National Highway Traffic Safety Administration. Motor vehicle fatalities are limited to occupant fatalities and exclude related fatalities to pedestrians, bicyclists, and others. On average, including fatalities to other than motor vehicle occupants in motor vehicle accidents would add approximately 5,500 fatalities to the motor vehicle fatality total. Large trucks are defined as having a gross vehicle weight greater than 10,000 pounds. Truck related fatalities are also counted in the overall motor vehicle category. FHWA-RD-89-013, Present Practices of Highway Transportation of Highway Material, Harwood and Russell, indicates approximately 5% of truck accidents reported to the FHWA involved trucks carrying hazardous materials. Applying this percentage to overall hazardous materials transportation yields a risk of approximately 260 fatalities related to general truck transportation risk apart from risks related to the particular hazards of the materials themselves.
cDeaths per passenger mile should also be considered as a basic risk measure when comparing risks amongst various modes of transportation. As the average number of passengers in an aircraft far exceeds the average number of passengers in a motor vehicle, the passenger mile risk of air carrier transportation is significantly less than that of motor vehicle transportation.
dThe fatality rate in currently approximately 1.3 fatalities per 100,000,000 vehicle miles in 1999-2003, or approximately 1 fatality per 77,000,000 mi. Another way of looking at this is that if a person drove approximately 770,000 mi in their lifetime (15,500 mi/yr for 50 years), there is approximately 1 in 100 chance that person will die as a result of an automobile accident during their lifetime.
eWISQARS (Web-based Injury Statistics Query and Reporting System) Injury Mortality Reports 1999-2003, Department of Health and Human Services’ Centers for Disease Control and Prevention. Only unintentional fatalities were used in this report. Fire data was limited to fire/flame fatalities and excluded fatalities due to contact with hot objects/substances.
fFatality data obtained from the Census of Fatal and Occupational Injuries, Department of Labor’s Bureau of Labor Statistics (2003 and 1999-2002) Workforce data obtained from the Current Population Survey, Department of Labor’s Bureau of Labor Statistics. Workforce risk calculated using the total employed civilian work force.
gNational Transportation Statistics, Department of Transportation’s Bureau of Transportation Statistics. Railroad fatality statistics include railroad only fatalities and grade crossing fatalities. Mileage data used was for Railroad System Safety and Property Damage Data.
hBoating Statistics—2003, United States Coat Guard.
iInjury Facts, National Safety Council. 2004, 2005/2006, and 2007 editions used to compile data.
jNational Transportation Statistics, Department of Transportation’s Bureau of Transportation Statistics. Air carrier data was calculated for all air carriers operating under either 14 CFR 121 or 14 CFR 135. Data used in this comparison was from air carriers operating under 14 CFR 121, which includes large aircraft, and under 14 CFR 135, which includes aircraft with less than 10 seats. Passenger and cargo aircraft are included in both categories.
kOther than the persons aboard the aircraft who were killed, fatalities resulting from the September 11 terrorist acts are excluded.
lU.S. Natural Hazard Statistics, National Weather Service. The National Weather Service is a program of the Department of Commerce’s National Oceanic and Atmospheric Administration (NOAA).
mHazardous Materials Incident Data, Department of Transportation, Pipeline and Hazardous Materials Safety Administration. http://hazmat.dot.gov/riskmgmt/riskcompare.htm.
There is often a disconnect between the measured safety aspects of aviation and the perception among the public and press of the apparent risks involved.
In 1997, the White House Commission on Aviation Safety and Security issued a challenge to the FAA and the aviation industry—to reduce the air carrier fatal accident rate by 80% in 10 years. The 2007 partial data to date reveals a rate of 0.19 fatal accidents per 100,000 departures—a 63% reduction. The draft FAA strategic plan for the period 2008 to 2011 has set goals for safety in the NAS using aircraft departures as the exposure measure:
Introduce a new performance metric for commercial air carrier safety—fatalities per 100 million enplanements and reduce the current measurement to half by 2025
Overall aircraft accident rate—reduce the rate per aircraft departure
Fatalities and losses by type of accident—reduce the number and type of fatalities and losses from accidents that occur for each major type of accident
Occupant risk—reduce the risk of mortality to a passenger or flight crewmember on a typical flight
On November 21, 1988, the FAA published its final drug-testing rules: Anti-Drug Program for Personnel Engaged in Specific Activities. Breath alcohol testing was required a few years later. These rules require operators under the Code of Federal Regulations (CFR) Parts 121 (air carrier) and 135 (commuter/air taxi) to establish antidrug programs for employees (including pilots) who perform safety-related functions (6). More than 500,000 aviation employees are affected by this program, which requires alcohol testing, and urine testing for five commonly abused drugs: marijuana, cocaine, opiates, amphetamines, and phencyclidine (PCP). Testing program results have shown a low rate of positive drug test results in aviation from the beginning of the testing program, especially among flight crews. In 1991, FAA statistics from drug tests conducted on 279,881 aviation employees and job applicants in safety- and security-related positions showed that 0.96% of the test results were positive for drugs of abuse, and in 1992, the rate was 0.95%. Those testing positive included repair facilities workers, contractors, and airline personnel and applicants. The positive rate for airline employees and applicants remained approximately the same in 1991 (0.46%) as in 1990 (0.40%).
Preemployment tests accounted for 49% of the positive results in 1991 and 44% in 1992. Random tests of current employees accounted for the 46% of the positive results in 1991 and 50% in 1992. Return to duty, reasonable cause, and periodic tests, in that order, accounted for the remaining positive results in 1992. There were no positive postaccident test results in 1992, and four in 1991. Positive results from random tests remained below 1% for the third consecutive year. Flight crew accounted for 42 positive results in 1991 and 32 in 1992. By far the largest numbers of positive test results come from maintenance personnel (1,586 in 1991 and 1,598 in 1992). Positive results for both years indicated that marijuana was most prevalent (52% in 1991 and 57% in 1992), followed by cocaine (42% in 1991 and 33% in 1992), amphetamines (4% in 1991 and 4.7% in 1992), opiates (5% in 1991 and 4% in 1992), and PCP (1% in 1991 and 0.7% in 1992). Some persons tested positive for more than one drug. Clearly, progress has been made, and the aviation industry has now been permitted to reduce the random drug test rate to 25% of covered employees.
In the fall of each year, the Federal Register contains a notice published by the FAA Federal Air Surgeon pursuant to 14 CFR Part 121, Appendix I, Section V.C The notice will report the FAA Administrator’s decision on whether to change the minimum annual random drug-testing rate based on the reported random drug test positive rate for the entire aviation industry. If the reported random drug test positive rate is less than 1.00%, the Administrator may continue the minimum random drug testing rate at 25%. The notice published in the fall of 2006 contained data from 2005, where the random drug test positive rate was found to be 0.58%. Therefore, the minimum random drug-testing rate was published to remain at 25% for calendar year 2007. Similarly, 14 CFR Part 121, Appendix J, Section III.C, requires the decision on the minimum annual random alcohol testing rate to be based on the random alcohol test violation rate. If the violation rate remains less than 0.50%, the Administrator may continue the minimum random alcohol-testing rate at 10%. In 2005, the random alcohol test violation rate was 0.16%. Therefore, the fall 2006 publication [FR Doc. E6-18726 Filed 11-6-06; 8:45 AM] contained the announcement that the minimum random alcohol-testing rate would remain at 10% for calendar year 2007.
Cases
In July 2006 in Bullhead City, Arizona, a fatal accident with two fatalities and one serious injury during a general aviation operation in a Bonanza G36, was attributed by the NTSB in May 2007 to the pilot’s misjudged distance and speed that led to a long landing, and his inadequate recovery from a bounced landing. The accident was due to impairment from alcohol consumption that resulted in an in-flight collision with terrain during an aborted landing attempt. A contributing factor was the FAA‘s failure to identify existing evidence of substance (alcohol) dependence in the pilot due to an inadequate and incomplete process of screening medical applications (NTSB Identification: LAX06FA243).
In Unalaska, Alaska on January 2001, an accident that killed both pilots involved a DC-3 being operated as a nonscheduled air taxi and commuter (14 CFR 135) flight. The NTSB probable cause of October 2002 listed the airplane flight crews’ failure to maintain adequate distance/altitude from mountainous terrain during a departure climb to cruise flight, and the captain’s impairment from drugs. Factors in the accident were dark night conditions, and the first officer’s impairment from drugs. (NTSB Identification: ANC01FA033).
In June 2004, in Kodiak Alaska, a fatal accident involving a Beech C-45H Expediter during a nonscheduled air taxi and commuter flight resulted in the NTSB probable cause of September 2005 listing the pilot’s failure to follow proper instrument flight rules (IFR) procedures by not adhering to the published missed approach procedures, which resulted in an in-flight collision with tree-covered terrain. Factors contributing to the accident were a low ceiling, fog, rain, and the insufficient operating standards of company management by allowing unauthorized single-pilot instrument flight operations. Additional factors were the pilot’s impairment from cocaine, alcohol, and over-the-counter medication for cold, and the FAA‘s inadequate medical certification of the pilot and follow-up of his known substance abuse problems. (NTSB Identification: ANC04FA063).
There are some earlier examples as well. In January 1988, a commuter airliner crashed, killing the 2 crewmembers and 7 of the 15 passengers. The NTSB found that the captain was medically unqualified to serve as a crewmember on the flight due to his use of cocaine before the accident, and that his performance was degraded due to the adverse effects of his use of cocaine before the accident. This degradation was documented as contributing to the accident (7). In 1995, a small cargo aircraft flying under CFR 135 had a fatal crash after the pilot mishandled the engines; the NTSB found the pilot was impaired by the ingestion of alcohol (8). In spite of these cases, the random drug testing of flight crew employees has clearly indicated that they have a very low incidence of positive tests. This has led some analysts to point out the questionable cost-effectiveness of the program. However, the value of such testing as a deterrent has not yet been defined. Medication usage, and particularly alcohol use, remains a significant issue for general aviation. However, private flying operations are not part of the drug-testing program.
AIR CARRIER ACCIDENTS AND SAFETY
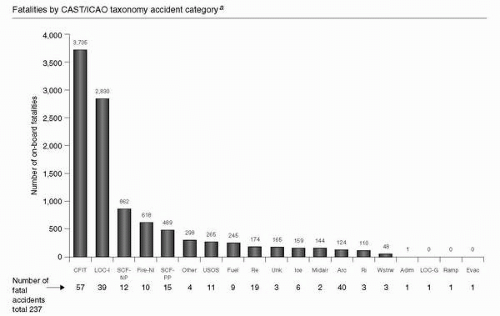
During the last decade, there have been two categories of loss of life in worldwide airliner operations that have been associated with the vast majority of airline fatalities. These have been controlled flight into terrain (CFIT) and loss of control in-flight (LOC-I) (Figure 25-5). With CFIT, there is the potential not only for primary prevention, but also of secondary prevention due to survivability and crashworthiness capabilities of large commercial aircraft. Because the impact is controlled, there is some predictability as to the angle of impact, aircraft attitude, and impact forces. The LOC-I, however, can be addressed only by primary prevention. In both cases, human performance issues figure primarily in the accident sequence of events. The response has been to improve pilot training in upset recovery techniques and to install enhanced ground proximity warning systems that give much improved and earlier warning and directional guidance in terrain alerting compared with earlier generation warning systems. The cost, size, and weight have been reduced for these systems to enable their use in commuter and general aviation aircraft. In addition, the Automatic Dependent Surveillance Broadcast (ADS-B) (http://www.ads-b.com/, http://www.adsb.gov/) is a set of technologies pioneered in Alaska with the Capstone project to markedly improve the safety and efficiency of aviation operations.
FIGURE 25-5 Worldwide fatal accidents and number of deaths by category of accident, 1987 to 2005. CFIT, controlled flight into terrain; LOC-I, loss of control-inflight; Fire-NI, fire-nonimpact; SCF-NP, system compund failure or malfunction-nonpowerplant; SCF-PP, system compund failure or malfunction-powerplant; RE, runway excursion; Unk, Unknown; ARC, abnormal runway contact; RI, runway incursion; WSTRW, windshear or thunderstorm; Adrm, Aerodrome; LOC-G, loss of control-ground; RAMP, ground handling; Evac, evacuation. (Boeing safety data, May 2006.)
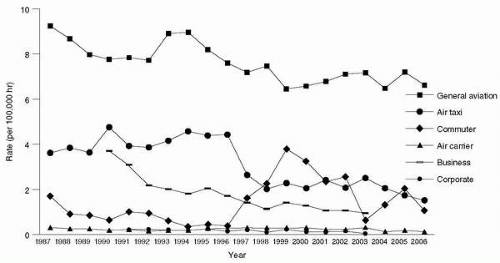
In Figure 25-6 the general aviation operations are governed under 14 CFR Part 91, the air taxi and the commuter operations are ruled under 14 CFR Part 135. The air carriers operate under 14 CFR Part 121. Business and corporate aviation could be operating under any of Part 91, 135, 121, depending on how they conduct their flight operations. A comparison of the overall annual accident rates per year by type of aviation operation illustrates the large difference between general aviation and scheduled air carrier operations by almost a factor of 10 (Figure 25-6). All of the aviation operations are showing improvement in accident rates over the period 1987 to 2006. The apparent increase in commuter accident rates in the late-1990s is due to a change in the definition and regulation of such operations. In March 1997, the definition of Part 121 operations changed. Before the change, scheduled aircraft with 30 or more seats were operated under Part 121 and those with less than 30 seats were operated under Part 135. After the change, scheduled aircraft with ten or more seats were classified as Part 121 operations; therefore, since 1997, most of the larger, turboprop carriers that were once popularly known as commuters now operate under Part 121. The regulatory change unmasked the commuter accident rate for the smaller and somewhat less safe unscheduled operators as the largest and safest commuter operators were merged into Part 121 operations. As time has passed, the relatively rapid increase in commuter accident rate was followed by a steady downward trend after the regulatory change. Also note that the growth of corporate/executive operations is essentially as safe as the scheduled air carriers. We are currently in a phase where the safety rate of scheduled air operations is the best it has been in aviation history.
FIGURE 25-6 Comparison of Accident Rates for 1987 to 2006 by type of aviation operation (NTSB, NBAA safety data).
AIR CARRIER SURVIVAL FACTORS
Regulations require that before every flight all passengers receive a safety briefing. Although it may be very short for a general aviation flight, airline passengers receive a more extensive and somewhat standardized demonstration by cabin crew or by prerecorded video relating to seat belts, passenger oxygen masks, cushion or flotation device usage, and location of emergency exits. Airline passengers also have a safety information card located near their seat that they are encouraged to read before each flight. Passengers seated in exit rows must meet certain FAA criteria or need to be reseated to ensure that someone sits near the overwing exits who is capable of operating the exits with minimal cabin crew assistance in case of an emergency evacuation of the aircraft. As part of the medical aspects of accident investigation during the postcrash investigation, attention should be directed to such circumstances of the accident sequence or those aspects of the cabin that helped or impeded evacuation of passengers. A survival factors group should be formed to study the consequences of the accident, and to document the successes and failures of the equipment and procedures for dealing with the postcrash environment. Survival factors is a multidisciplinary group comprising evacuation specialists, cabin safety investigators, physicians, flight attendants, and safety engineers, whose investigatory scope should include the items in Table 25-3 according to the NTSB Survival Factors Investigation Checklist and Outline (9).
The NTSB held a public meeting on February 21, 2001, to present safety report NTSB/SR-01/01: Survivability of Accidents Involving Part 121 U.S. Air Carrier Operations, 1983 through 2000. In all accidents involving U.S. air carrier flights (cargo and passenger) operating under Title 14 CFR Part 121, 1983 through 2000, there were 568 total accidents in which 71 accidents (12.5%) were fatal. As related to number of occupants, 51,207 occupants (95.7%) survived, whereas 2,280 occupants (4.3%) died. In 528 (93.0%) out of the 568 accidents more than 80% of the occupants survived. In 26 serious Part 121 accidents (those involving fire, serious injury, and either substantial aircraft damage or complete destruction), there were 2,739 occupants; 1,524 (55.6%) of those occupants survived, 716 (26.1%) died from impact, and 131 (4.8%) died from fire/smoke inhalation. In 12 (46.2%) out of those 26 serious Part 121 accidents, more than 80% of the occupants survived. In 19 of those 26 serious Part 121 accidents that were categorized as survivable, 1,523 of the 1,988 occupants (76.6%) survived, 306 (15.4%) died from impact, and 131 (6.6%) died from fire. In 12 (63.2%) of these 19 survivable serious Part 121 accidents, more than 80% of the occupants survived.
The report concluded that public perception of survivability may be substantially lower than the actual rate of 95.7% for all Part 121 accidents. Overall 96% of passengers survive all accidents, 56% survive serious accidents, and 77% survive serious-survivable accidents. Finally, Safety Board recommendations to passengers to improve their chances of survival include (a) plan escape routes to more than one exit, (b) pay attention to safety briefings by cabin crew, (c) read safety briefing cards provided at each seat, and (d) follow crew instructions (4).
TABLE 25-3
Survival Factors Checklist
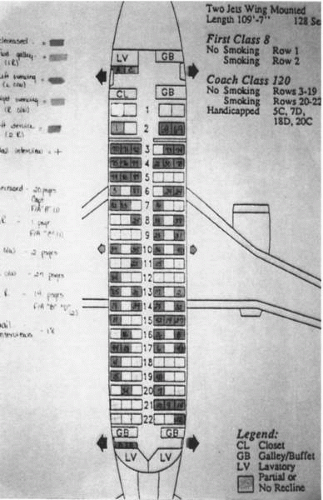
Airplane configuration
Including a diagram showing seating configuration, galleys, exits, location of emergency equipment, etc.
Crew and passengers information
Including cockpit, cabin crew, and passenger interviews. Cabin crew interviews should collect information related to seatbelt and shoulder harness integrity before and after impact, difficulties during escape, description of injuries and how they were sustained, how flight crew evacuated the airplane, etc.
Airplane damage and wreckage site
Including description of terrain, site, distance, heading, and relative bearing of ground scars and air conditioning components from main wreckage; description of obstacles/structures struck. Airplane Damage, including description of the airplane damage as it relates to fire pattern, egress, fuselage and wing crush, etc.
Emergency systems
Including the condition of personal announcement system, oxygen equipment, flashlights, first aid kits, megaphones, emergency lighting systems, evacuation alarm system, emergency escape slide, or slide/raft; condition and location of life rafts and life vests.
Evacuation
Including information related to: numbers of doors opened, number of slide/rafts successfully deployed and inflated, development and propagation of fire and smoke, deformation of the cabin, group behavior during the emergency, operation of the emergency floor lighting, operation by the crew of their protective and safety equipment, functioning and coordination of the cabin crew in the emergency, configuration of the seats, functioning of the fire-blocking materials, aisle widths, access to and capability of the exits to allow passengers to exit the aircraft.
Medical and pathological information
Including a summary of injury sustained (fatal, serious, minor, none and total, according to NTSB 49 CFR 830.2 Definitions) as well as a general description of the survivors’ injuries. Postmortem examinations:
Each crewmember must be positively identified
Postmortem examinations should be made on each cockpit occupant
Postmortem examination should be made on flight attendants, passengers, and persons on the ground as the circumstances of the accident indicate
Gross injury descriptions should include all fractures, dislocations, lacerations, amputation, burns, and condition of clothing
Toxicologic and microscopic examinations should be performed on all cockpit occupants, selected flight attendants and passengers, and other selected victims as the situation warrants
Emergency Response
Including search and rescue (SAR) information, Aircraft rescue and fire fighting (ARFF) response:
Dispatch and Communications, Fire Suppression, and Rescue Activities
After action activities
Law enforcement response, medical response, disaster preparedness, and airport certification
GENERAL AVIATION ACCIDENTS AND SAFETY
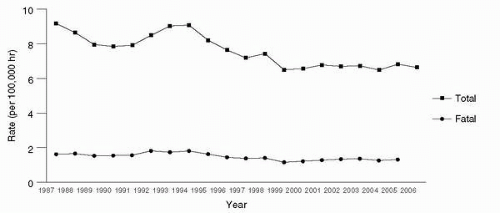
Safety records from 1938 to date chronicle almost 70 years of general aviation having an improving safety record with approximately an 18-fold decrease in total accident rate. The decline in the fatal accident rate for general aviation has been slower with perhaps a ninefold decrease over the same time period. The last 20 years show a slower decline in the United States (Figure 25-7) with a 26% decrease in the total accident rate and a 20% decrease in the fatal rate. The General Aviation Manufacturers Association maintains some general aviation data for other countries on their website (http://www.gama.aero/home.php). Although all forms of aviation operations will benefit from improved crashworthiness and accident prevention, the greatest number of lives lost in aviation is still in general aviation operations; therefore there is a need to concentrate safety resources on general aviation safety research to continue the improvement in the accident rate.
GENERAL AVIATION ACCIDENT PREVENTION
The efforts of the FAA Office of Aerospace Medicine to initiate an extensive education program for general aviation pilots regarding medical factors of accident prevention almost three decades ago do contribute to the improving GA accident rate in Figure 25-7. This educational program included significant safety enhancements through a nationwide effort to draw attention to the common causes of accidents and in particular the medical and human factors aspects common to mishaps. In this program, general aviation pilots were made aware of the effects of hypoxia as well as other safety information usually taught to military pilots by the use of military hypobaric chambers and crews. Many thousands of private and commercial pilots have participated in this training. As FAA flight standards and Air Traffic Control (ATC) accident prevention procedures were added to the curriculum, the interest increased, and this regional recipe for accident prevention through education was provided nationwide. Currently, every FAA general aviation district office or flight standards district office has an accident prevention specialist (APS). The practitioner of aviation medicine can obtain valuable assistance through the services of the APS, who has excellent teaching aids, including a Barany chair to demonstrate the greatest single cause of fatal general aviation accidents, spatial disorientation. Excellent aeromedical teaching materials for the FAAAME are also available from the FAA‘s CAMI at Oklahoma City and these materials have been disseminated to many other countries (http://www.faa.gov/pilots/training/airman education/).
FIGURE 25-7 General aviation accident data for 1987 to 2006 from the General Aviation Manufacturers Association (FAA and National Transportation Safety Board data).
GENERAL AVIATION CRASHWORTHINESS
Most aviation fatalities and serious injuries occur in general aviation operations. Serious injury refers to any injury that meets the following criteria (1):
Requires hospitalization for more than 48 hours, commencing within 7 days of the date of receiving the injury
Results in a fracture of any bone (except simple fractures of fingers, toes, or nose)
Causes severe hemorrhages, nerve, muscle, or tendon damage
Involves any internal organ
Involves second- or third-degree burns, or any burns affecting more than 5% of the body surface
In examining accidents in one decade alone, more than 100,000 occupants were injured in approximately 40,000 accidents. Of these accidents, 17.7% involved at least one fatality. The NTSB accident investigators report that few changes have been made in cabin interior design or restraint systems, which might have eliminated or reduced these injuries. Sharply contrasting with this is the progress in improving air carrier and automobile crashworthiness. Automobile accidents have only one fatality for every ten serious injuries, whereas general aviation aircraft accidents produce two fatalities for every three serious injuries. Aircraft impacts have greater speeds and therefore have much more energy to dissipate, because energy is proportional to the square of the speed.
The NTSB acknowledges that automotive and aircraft accident statistics are not directly comparable because of the higher speeds and many different crash loads and vehicle design objectives in aviation. The NTSB references to crashworthiness remark that when crash forces transmitted to occupants through properly designed seats and restraint systems do not exceed the limits of human tolerance to abrupt deceleration, and when the cabin structure remains sufficiently intact to provide a livable space immediately around the occupants, crew and passengers should survive the accident without serious injury (10,12). The postcrash environment may contain other lethal potentials such as drowning or weather-related hazards that the pilots and their passengers may have to surmount. Therefore, survival training for wilderness exposures is a reasonable precaution that all pilots should undertake.
In an effort to improve crash survivability through crashworthy design, engineers developed the “CREEP” concept (see subsequent text). Crashworthiness is defined as the ability and technology of an aircraft and its internal systems and components to protect occupants from injury in the event of a crash. In other words, crashworthiness does not prevent the accident from happening; it rather mitigates the effects of the impact and therefore changes favorably the injury outcome.
Hugh DeHaven is considered to be the “father” of crashworthiness for his work in protective design and injury biomechanics at Cornell University Medical College in the early 1930s. He started the viewpoint that “airplane crashes should be studied from the point of view of accident pathology and injury causes” (13). He also conducted the combined engineering and pathological review of natural experiments from attempted suicide jumps from 50 to 150 ft in survivors. Impact velocities, stopping distances, and estimates of impact forces were closely determined, providing valuable data to his crash injury research.
The acronym “CREEP” has been used as a systematic tool to organize the important aspects/factors of crash survivability as follows:
C = Container, related to the occupants’ “living space” during the impact
R = Restraint, dealing with restraint systems and equipment provided to crew and passengers
E = Energy absorption, directly related to the deceleration forces transmitted to the occupants through the aircraft structures
E = Environment, related to the “internal” surrounding environment of crew and passengers
P = Postcrash factors, mostly related to the rapid evacuation of the aircraft and the postimpact conditions such as fire, water, and hostile terrain
A detailed analysis of these factors is beyond the scope of this chapter; however, it is worth mentioning the similarities to the epidemiologic approach postulated by William Haddon Jr. The Haddon Matrix was developed in an effort to develop a strategy for injury identification and control. Such a matrix “provide(s) a means for identifying and considering, cell by cell: a) prior and possible future allocations and activities, as well as the efficacies of each; b) the relevant research and other knowledge—both already available and needed for the future; and c) the priorities for countermeasures, judged in terms of their costs and their effects on undesirable injury results, that is on the problems to be reduced” (14). In its simplest form, the matrix has two dimensions: The first is what Haddon called phases. In the case of aircraft accidents, the phases are “precrash,” “crash,” and “postcrash.” The second dimension of the matrix is divided into three factors: the “human,” (or host, i.e., the person susceptible to injury; the specific agent), the “vehicle” (or “vector” transferring the mechanical energy), and the “environment” (which can be subdivided into “physical” and “sociocultural”).
Because of the volume and complexity of data in aircraft accident investigation, it is necessary to develop a database system to process and analyze injury data in a meaningful way. The Haddon matrix might be successfully used for the purpose of evaluating intervention measures aimed to reduce injuries if sufficient detailed injury data was gathered from accident investigations. This information is not currently collected in detail apart from the major accident investigations involving the Washington based go-team investigations, where a Survival Factors group is formed.
To determine an injury pattern, it is necessary to correlate injury information with the following basic information: (15).
The impact forces (direction and magnitude of accelerative forces)
The time, duration, and direction of the applied forces
The cockpit or cabin configuration
The nature of the accident and subsequent occurrences and
The occupant kinematics in the accident, particularly relating to restraint systems and evacuation methods
In addition, during impact there are simultaneous rotational and translational movements of the different body parts (i.e., head, neck, thorax, abdomen, and upper and lower extremities). The biodynamics of these moving body parts during impact forces are very complex and not well understood (16). Collection and analysis of good quality injury data in real aircraft accidents and modeling with slide crash test data should answer questions concerning injury patterns. For example, a detailed evaluation of seat damage, including cross validation using injury data has been proposed. Seat structural performance can indicate the appropriateness of existing dynamic test severity levels and can assist investigators in estimating crash severity. In addition, injury patterns can be used to evaluate the adequacy of occupant injury assessments made during dynamic tests. Integration of seat structural performance and injury data is crucial to form a basis for developing new safety standards and refining existing standards (DeWeese R, personal communication, 2006, FAACAMI).
The unique nature of injury data constitutes a real challenge to injury researchers in reference to methodological issues, etiology, and the impact of interventions in the field of injury prevention and control (14,17). Some examples of the complicated characteristics of injury data are summarized as follows:
Injuries occur in the context of a sudden transfer of physical energy, either mechanical, thermal, radiant, chemical, or electrical. In the case of aircraft accidents, moving objects are vehicles of mechanical energy.
Injuries might occur more than once to the same individual.
A single event such as an aircraft accident might result in multiple types of injuries to multiple body sites with different severities.
Knowledge, attitudes, and behaviors play a major role in determining the etiology of injury.
Determining the mechanisms of injuries is a critical step in developing injury prevention and mitigation strategies in aviation accidents. Developing a research-oriented database to categorize and classify injury outcome in aircraft accidents is the next step needed to answer fundamental questions related to injury causation (18).
In Section 23.785 of 14 CFR Part 23, as amended by Amendment 23-19, effective July 18, 1977, the FAA required shoulder harnesses (front seat) for all normal, utility, and acrobatic category airplanes for which an application for a type certificate was made on or after July 18, 1977. It also requires all small civil airplanes manufactured after July 18, 1978 to have an approved shoulder harness for each front seat. In FAA policy statement, ACE-00-23.561-01, regulatory guidelines for the approval of the retrofit of older aircraft with shoulder harnesses have been published. The advent of airbags being incorporated into aviation restraint systems is becoming very widespread and most new aircraft are sold with this option. The investigator should be aware of Advisory Circular AC 21-34, Shoulder Harness-Safety Belt Installations, June 4, 1993.
An older study ending in 1952 still holds valuable lessons because there are many general aviation aircraft that still utilize older style restraint systems. The study reported that of 913 accidents involving 1,596 occupants and 15 aircraft models, there were 389 fatalities, and that “roughly one third of the 389 people that were killed … died unnecessarily.”
The most common deficiencies in general aviation aircraft are as follows:
Lack of adequate upper torso restraint. Head injuries remain the most frequent injury as well as the major cause of death and serious trauma. This usually occurs when the occupant jack-knifes over the seat belt and contacts hard, sharp, unyielding, or rigid structures.
Inability of seats to adequately attenuate vertical compressive forces. Recent attention has been given to improved design of the front seats, but the rear seats do not appear to provide equivalent protection.
Lack of adequate seat support and attachment. Even with upper torso restraint and attenuated vertical compressive forces, an inadequately supported and attached seat will reduce injury tolerance.
Cabin interiors that contain many lethal surfaces, structures, and objects that cause death or serious trauma upon crash impact. Flailing appendages, even when upper torso restraints are worn, can contact controls and nonyielding structures.
An FAA report states that, “Severe but nonfatal injuries were common in 3 to 5 G accidents. Fatalities and very severe injuries occurred in crash decelerations of 6 to 10 G. At 10 G and above, most present general aviation aircraft disintegrate to the extent that the value of restraint equipment for crash survival is doubtful.” In contrast, a new-generation agricultural aircraft was manufactured, patterned after a prototype aircraft with a 50-G seat, an integral double upper torso restraint with inertial reel, a 40-G cockpit box, the storage hopper placed between the engine and the pilot to provide energy absorption, and an overturn structure (roll bar). In a 10-year period, these aircraft were in 368 accidents with only 3% fatalities, whereas for the same period, the fatality rate in all U.S. general aviation aircraft averaged 12.8%. If all occupants wear shoulder harnesses, fatalities might be reduced by 20%. Of seriously injured persons in survivable crashes, 88% are expected to experience significantly fewer life-threatening injuries if shoulder harnesses are worn. Thirty-four percent of the seriously injured occupants of survivable accidents are expected to be less seriously injured if energy-absorbing seats are available (10,12).
Flying as either a passenger or crewmember is associated with a measurable degree of risk. This risk has continued to decrease as accident prevention, protection, and survival is improved. If government, manufacturers, airport personnel, crews, and passengers continue to contribute to, and use, the knowledge, equipment, training, and information available, the probability of survival is excellent should an accident occur. Professor Jim Reason developed a model of human error that at its center states that although the expression of human error seems almost infinite in variety, it actually reduces down to several overall categories of errors, omissions, and mistakes. His other important insight was that the sequence of events that link up together to result in an accident can span many scales of time and that there are some latent or hidden deficiencies in aerospace systems that may contribute in unexpected ways to the causation of accidents. There are a number of barriers preventing an accident, each capable of trapping a sequence of events that otherwise would lead to an accident. These barriers stack up in layers and because there are no perfect safety programs there are “holes” in each layer of accident prevention or safety layer. This is why the model is also known as Reason’s Swiss cheese model of human error (19). Aviation accidents are rare because the complex system of aerospace operations has multiple layers of safety; therefore, while deviations, mistakes, and failures may not be all that rare, it is extremely rare that a sequence of events (or misevents) can proceed all the way to an accident occurrence. Each of these layers is “peopled” by the various individuals in aviation, from the owner/operator of the aviation enterprise, through the regulatory and inspection authorities, the aircraft designers, manufacturers, mechanics, dispatchers, air traffic controllers, flight attendants, and pilots. Therefore everyone in aviation, in each layer, can alter the chain of events as described by Reason’s human error, and can prevent accidents. The aerospace medicine practitioner has several opportunities to actively intervene in and contribute to aviation operations to prevent accidents. These include being a source of education for aircrew regarding aviation stressors, aerospace human factors and by providing proper medical certification of pilots. When an accident or incident occurs, aerospace medical practitioners also have many skills to offer to the investigation of the sequence of events that culminated in the accident or incident.
MEDICAL AIRCRAFT ACCIDENT INVESTIGATION TECHNIQUES
Aircraft accidents are not new occurrences. With the first flights of humans came the first flight accidents of humans. An accident badly damaged the front rudder frame of the Wright Flyer, cutting short the early flights of Wilbur and Orville Wright in the first successfully controlled, powered, and manned heavier-than-air machine near Kitty Hawk, North Carolina, on Thursday, December 17, 1903. Analysis of accidents leads to continued improvement and refining of aircraft design and the discovery of piloting techniques. Although this chapter uses aircraft accidents to illustrate the techniques for the investigation of accidents, identification of victims, and evaluation of injuries, the methods are directly applicable to accidents involving other modes of transportation.
History
The first reported aircraft fatality in the United States occurred during acceptance flights when Orville Wright took an observer aloft to test a new propeller while demonstrating the Wright Type A Flyer to the U.S. Army Signal Corps at Fort Myer, Virginia, on September 17, 1908. When a crack developed in the starboard propeller of the Flyer, causing violent vibrations and failure of the elevator, the aircraft, from an altitude of approximately 75 ft, impacted the ground (Figure 25-8). First Lieutenant Thomas E. Selfridge, a pilot candidate, aboard as the observer, died as a result of a compound comminuted fracture of the base of his skull during the crash. An autopsy was performed, and Captain H. H. Bailey (Medical Corps, U.S. Army) determined the cause of death. An aeronautic board investigated to determine the cause of the crash and produced a summary report, which interestingly did not address head injury protection. The next pilot candidate, Lieutenant Hap Arnold, began to wear a football helmet to provide some head protection and also pioneered the use of goggles.
FIGURE 25-8 Crash of the Wright Flyer at Fort Myer, Virginia, on September 17, 1908 (photo courtesy of Armed Forces Institute of Pathology).
On May 6, 1935, Transcontinental and Western Air flight no. 6, with Senator Bronson M. Cutting on board, crashed, killing five persons including the Senator. As a result of this crash, an outraged Senate quickly authorized the Committee on Commerce “to investigate … [the Cutting crash] … and any other accidents or wrecks of airplanes engaged in interstate commerce in which lives have been lost; and to investigate … interstate air commerce, the precautions and safeguards provided therein, both by those engaged in such interstate air transportation and by officials or departments of the United States Government; and to investigate … the activities of those entrusted by the Government with the protection of property and life by [sic] air transportation, and the degree, adequacy, and efficiency of supervision by any agency of Government including inspection and frequency thereof …” (20). This action established a federal interest in aircraft accident investigations that was initially included in the activities of the Civil Aeronautics Board, which in 1958 became the FAA, and in 1974 an independent body, the NTSB, was mandated by Congress to determine the probable cause of all transportation accidents, and to make safety recommendations to the regulating agencies and industry.
Although investigation into the mechanical causes of crashes progressed, and medical expertise accumulated during the World Wars I and II, it was not until the 1950s that the value of medical investigation of aircraft crashes became apparent. Several well-publicized and seemingly mysterious crashes of jet-powered British Comets, the first jet-powered commercial passenger aircraft, led to medical investigations that marked the beginning of modern aeromedical pathology, which we now call aerospace pathology. The investigations dispelled the sense of mystery regarding passenger jet transportation by providing thorough and scientific explanations for the sequence of events and the correlation of the postmortem findings with the flight environment and aircraft structures. One Comet crashed on January 10, 1954, with 35 persons on board approximately 25 minutes after taking off from Rome en route to London. Another Comet crashed en route to Cairo from Rome on April 8, 1954, with 21 persons on board. Both planes crashed at sea, and there were no immediate indications as to the cause. Postmortem examination of the remains of the passengers and crew who floated to the surface allowed pathologists to determine that an explosive decompression had occurred in these pressurized cabins. This structural failure resulted from insufficient hull strength to withstand the pressure differential between the cabin and the outside atmosphere at altitude due to the repetitive stresses of flight leading to metal fatigue (21).
The greatest loss of life in an aviation mass disaster was the collision of two Boeing 747 jumbo airliners at Tenerife in the Canary Islands on March 27, 1977. The 583 fatalities required a large and multinational, multidisciplinary response (Figure 25-9). This accident focused attention on the problems that aircraft accidents and other mass disasters can present and was partly responsible for the development of a human factors focus on crew resource management. One of the authors of an earlier version of this chapter, Dr Robert R. McMeekin was involved in the on-scene investigation.
FIGURE 25-9 Wreckage of two 747 airliners on the runway at Tenerife, Canary Islands, on March 27, 1977 (photo courtesy of Armed Forces Institute of Pathology).
ORGANIZATION OF THE INVESTIGATION
International Civil Aviation Organization Guidelines
Investigations are performed using ICAO‘s “International Standards and Recommended Practices, Aircraft Accident and Incident Investigation,” which is Annex 13 to the convention on International Civil Aviation. The guidelines are available on the Internet (www.icao.org).
The use of a multidisciplinary team approach to accident investigation leads to coordinated efforts in the following general groups of investigators: operations, structures, power plants, human performance, survival factors, medical factors, aircraft systems, witnesses, ATC, weather, flight data recorder (FDR)/cockpit voice recorder (CVR), maintenance records, airport rescue, and firefighting. Other groups are formed as necessary to deal with particular aspects of the investigation, and sometimes one group subsumes another group’s function and members.
Multidisciplinary Team Constitution
Modern investigations vary in their complexity and the need for specialized team members. In general, it is advisable to have identified, before an accident, individuals and organizations that are able to provide expertise to the investigation in a variety of specialized disciplines. Increasingly, multidisciplinary team makeup is necessary to deal with aviation disaster management and investigation. Forensic pathologists are essential to the documentation of the cause of death and injury patterns that will be learned from the autopsies. Aerospace pathologists will bring additional expertise to bear in survival factors investigations, and clinicopathologic correlation of the observed deaths and injuries. Forensic anthropologists are useful in bone fragment identification and classification. Forensic odontologists provide essential dental identification expertise for the on-scene phase of the investigation. DNA specialists and teams have become the standard in providing positive identification of fatalities, especially in high-impact crashes where large numbers of body fragments are recovered. Aerospace medicine specialists, particularly if they are also pilots, contribute their knowledge of aviation medicine, as well as human factors, pilot skills, and the impact of medical factors on human performance. Aviation human factors psychologists bring essential skills in understanding human performance in areas of pilot cognition, ergonomics, and in using specialized techniques such as voice stress analysis. An image specialist with training in aircraft accident investigation can provide essential documentation using print, slide film, and videotape, as well as digital media. This team member frees up the other specialists to deal with their specific involvements. Some areas overlap, and not all disciplines are available for every accident.
The NTSB will designate one or more team members representing the various qualified parties of the investigation to be assigned to each of these areas, but the actual composition of the accident investigation team always depends on the circumstances of the accident and the number of people involved. For example, human factors, survival factors, and medical factors teams may be combined or maintained separately. The survival factors/medical factors group considers the crashworthiness aspects of the investigation, with particular emphasis on organization, identification, injury tolerance, and analysis of injury patterns, and also deals with the morgue and the local jurisdiction. The human performance group examines factors that affect the performance of the flight crew, mechanics, and air traffic controllers, and their investigation evaluates the cognitive, ergonomic, and psychological factors that may have contributed to the accident. All these specialized groups’ observations are the basis of recommendations for changes in standards for training, medical certification, and selection of the various professions. They also lead to improvements in cockpit or passenger compartment layout and the design of avionics, seats, restraints, protective equipment, and escape mechanisms and pathways. More recently their observations have implications for organizational inputs to accident causation by highlighting supervisory and organizational aspects of airline operation and regulation that may have contributed actively or latently to the chain of events leading up to the accident.
Jurisdiction
The jurisdiction to conduct investigations of deaths usually rests with the government of the territory in which the death occurs. Treaties, conventions, and executive agreements resolve many of the problems that result from differences in laws among countries. The 1944 Chicago Convention provides for international participation by the state of registry in investigations of civil aviation accidents as follows (22):
In the event of an accident to an aircraft of a contracting State occurring in the territory of another contracting State, and involving death or serious injury, or indicating serious technical defect in the aircraft or air navigation facilities, the State in which the accident occurs will institute an inquiry into the circumstances of the accident, in accordance, so far as its laws permit, with the procedure which may be recommended by the International Civil Aviation Organization. The State in which the aircraft is registered shall be given the opportunity to appoint observers to be present at the inquiry and the State holding the inquiry shall communicate the report and findings in the matter to that State.
Effective international cooperation resulted when a major air disaster involving two Boeing 747s occurred in Tenerife in the Canary Islands in 1977. U.S. representatives participated in the investigation, and the Spanish government permitted the removal of the fatally injured U.S. passengers from Tenerife to Dover Air Force Base in Delaware for identification.
Jurisdiction disputes also occur at the functional level between government agencies. The NTSB, Federal Bureau of Investigation (FBI), and Department of Defense (DoD) are only a few of the U.S. agencies with an interest in accident investigation. In addition, the Environmental Protection Agency (EPA) is involved, ensuring the cleanup of the accident scene. The Occupational Safety and Health Agency (OSHA) has determined that blood-borne pathogen training is required for accident investigators, on-scene exposures are properly followed up and documented, and that accident investigators be offered vaccination against hepatitis B infection. Although their interests may occasionally be diverse, personnel from the agencies are able to work together harmoniously. Statutes, regulations, and letters of agreement covering most situations clearly define the relationships between the various federal agencies.
In the United States, by virtue of the 10th Amendment to the Constitution, the individual states retain jurisdiction over matters that federal legislation has not preempted. State laws regarding postmortem investigations differ considerably, and the official who authorizes postmortem examinations varies from state to state. Autopsy is available in some states only when this official suspects that a death resulted from unlawful means. The NTSB, FAA, U.S. military services, and armed forces from many other countries recognize the importance of the pathologic and toxicologic investigation of fatal aircraft accidents, and they have published regulations requiring the postmortem examination of all fatally injured crewmembers. With respect to civil jurisdictions, the NTSB routinely obtains an autopsy on pilots and has toxicologic specimens sent to the CAMI for analysis. There are barriers to conducting comprehensive accident investigations, and the result is that many postmortem investigations of aircraft accident fatalities are inadequate.
Adequacy of Investigations
Investigations of aircraft accident fatalities are inadequate or unavailable in certain circumstances because understanding of the federal aims of the investigation and cooperation is lacking. Approximately 90% of U.S. military aircraft accident fatalities occur in areas where the federal government has no authority to obtain postmortem information that may be essential to aviation safety and accident prevention, and where many local officials refuse to fully cooperate with the military investigations. In states without a state medical examiner system, where each county is responsible for death investigation, there is often lack of a qualified staff to deal with a large-scale aircraft mass disaster. Even with smaller scale general aviation accidents, there is often little cooperation.
The primary objective, and the legal responsibility, of the investigating authority is in determining the cause of the accident, as well as documenting the consequences of the accident, including the reasons for death and injury of the crew and passengers. The primary interest, and legal responsibility, of coroners and medical examiners is in determining the cause and manner of death and seldom in collecting information concerning aircraft accident and injury prevention. The authorizing official or examining pathologist may have no interest in aircraft accidents and may have no knowledge, experience, or training in the techniques involved. These officials often conduct only an external description of the body, frequently omitting the microscopic and toxicologic examinations necessary to determine the presence of toxic substances in the aircraft and preexisting disease in the aircrew. Even when local officials have the authority to conduct complete autopsy examinations, they may elect not to perform them. In one instance, in answering a request for information about his investigation after a fatal aircraft accident, a coroner’s pathologist responded, “according to local interpretation of state law, a coroner’s autopsy precedes to [sic] the cause of death and is not an academic endeavor. When the cause of death is obvious in the gross autopsy, as is usually the case in aircraft accidents, microscopic examinations are not performed.” (McMeekin personal communication, 1985) In such cases, the military must depend on local civilian officials to conduct whatever examinations they deem advisable.
Even the presence of trained forensic pathologists with experience in investigating aircraft accidents does not ensure adequate examinations. Statutory authority often limits even these trained investigators in the scope of postmortem examinations. Most coroners and medical examiners do not have sufficient funds or staff to permit the more than 2 workdays often needed for a thorough investigation. Situations in which it is not clear who, if anyone, has jurisdiction are especially disconcerting because nothing is accomplished, although everyone agrees that postmortem examinations are needed. In the above-mentioned major air disaster involving two Boeing 747s at Tenerife, there were 583 fatalities, of which more than half were U.S. citizens. Of the 396 persons aboard the Pan American aircraft, 334 died. The jurisdiction of Spain to investigate the accident, and of the United States to participate, was clear under the provisions of the Chicago Convention. Logistics, however, necessitated the removal of the U.S. fatalities to Dover Air Force Base, where easier access to communications facilities aided the identification process. Detailed postmortem examination could have determined the exact cause of death and why so few survived this ground collision, but no one established the jurisdiction to conduct complete autopsy examinations. Without these examinations, the investigation was incomplete. The state of Delaware could not give adequate authorization for postmortem examinations because the deaths did not occur in Delaware. The NTSB did not have jurisdiction because Spain was in charge of the investigation. Everyone agreed that the investigations were necessary, but no one could cite a proper authority. The result was that the investigators used only those methods necessary to establish the identity of the bodies. Valuable information was lost that could have contributed to the furtherance of air safety.
Disaster Mortuary Operational Response Team
The Disaster Mortuary Operational Response Team (DMORT) is a federal-level response team designed to provide mortuary assistance in the case of mass fatality and cemetery-related events such as flood damage to a cemetery. The United States Public Health Service (USPHS) and the Office of Emergency Preparedness-National Disaster Medical System, along with thousands of volunteers from across the country dedicated to helping those in need, sponsor this and other medical teams. The Family Assistance Act of 1996 created a new division within the NTSB called the NTSBFamily Affairs Division, which is charged with helping local authorities to coordinate victim identification and family assistance. The NTSB has agreements with DMORT and other national entities that assist them in fulfilling their duties under this law. A memorandum of understanding between the NTSB and USPHS gives the NTSB and its Family Affairs Division the ability to request DMORT for all transportation accidents involving multiple deaths.
Federal Interest in Aircraft Accident Investigation
Congress has expressed an interest in the investigation of aircraft accident fatalities. The Federal Aviation Act of 1958, enacted on August 23, 1958, established the FAA. Other laws, notably by the Department of Transportation Act of 1967, subsequently amended this basic enabling legislation. On July 5, 1994, Public Law 103-272 recodified certain laws pertaining to transportation. As a result, provisions of Subtitle VII of Title 49, United States Code, superseded the Federal Aviation Act. The 1988 Aviation Safety Research Act, later recodified in Title 49 United States Code (49 U.S.C.), provides a mandate for CAMI to conduct civil medical accident investigations and research. Furthermore, Congress determined that the federal government has an overriding interest in aviation safety and enacted legislation to ensure thorough investigations, including autopsies, of all civil aircraft accidents. The Independent Safety Board Act of 1974 established an NTSB that was separate from the FAA. This act was also later recodified into 49 U.S.C. The NTSB may conduct these autopsies regardless of provisions of local law unless the local laws pertaining to autopsies are based on the protection of religious beliefs, as follows (23):
In the case of any fatal accident, the Board is authorized to examine the remains of any deceased person aboard the aircraft at the time of the accident, who dies as a result of the accident, and to conduct autopsies or such other tests thereof as may be necessary to the investigation of the accident: provided, that to the extent consistent with the needs of the accident investigation, provisions of local law protecting religious beliefs with respect to autopsies shall be observed.
A similar federal interest exists in military aircraft accidents in which the economic effects and impact on national defense are critical, but the authority of the NTSB does not extend to the investigation of accidents involving solely military aircraft. Statutes authorize the U.S. Army and Air Force to conduct autopsies of persons fatally injured onboard military aircraft when a fatal accident occurs on a military reservation where there is sole U.S. military jurisdiction. The military services recognize the importance of postmortem investigations of all fatally injured military crewmembers, and their regulations require autopsy examination regardless of where death occurred. Regulations give military commanders power, similar to that of coroners, to direct the performance of autopsies of aircraft accident fatalities involving military personnel.
The FAACAMI processes all toxicology samples obtained by the NTSB investigations and maintains an aircraft accident research team to provide multidisciplinary support regarding medical and human factors to the NTSB and the FAA Office of Accident Investigation. The Office of the Armed Forces Medical Examiner, located at the Armed Forces Institute of Pathology (AFIP), and staffed by fully trained forensic pathologists, investigates all fatal U.S. military aircraft accidents. The AFIP also provides consultation and pathology support to the NTSB and other government agencies. Active aviation pathology departments also exist in Germany, the United Kingdom, Spain, and other countries.
Phases of the Investigation
The success of the investigation depends on the degree to which one has prepared before the accident occurs. Usually the investigating authorities arrive after the immediate crash, fire, and rescue response from the affected airport/local community. Therefore, the preservation of life and immediate care of the ill and injured, as would be required in an airport disaster response plan, will not be considered here. The immediate postaccident period may seem chaotic, with many concurrent activities going on, all competing for attention by the medical accident investigator, and experienced investigators recognize the importance of the early development of an organizational plan that considers the following five general phases:
Preliminary evaluation
Data collection
Data analysis
Conclusions
Recommendations
The NTSB and CAMI have prepared autopsy guidelines for medical examiners to help guide their postmortem examinations. The Joint Committee on Aviation Pathology (JCAP) prepared an outline of six steps for the pathologist to take when investigating fatal aircraft accidents (24). These general steps are useful for participating in survival factor/medical factor investigations. These steps are an adaptation of the five investigation steps listed earlier, and they are useful guidelines for any investigating physician. Although no rigid protocol can describe in detail how to investigate all accident types that a pathologist may encounter, JCAP recommends the following steps for the investigation of injuries sustained by the victims of a crash.
The first step in the investigation is for the pathologist to familiarize himself or herself thoroughly with the type of aircraft, its internal structure, seating arrangement, ejection mechanism, and general layout, and, if possible, to examine an intact plane of the type in question. It is essential to review the location and operation of the cockpit and cabin crew safety equipment, the particular interior configuration of the cabin, which is usually different for different airlines even using the same make and model of airliner, and with the location and configuration of the emergency exits. An exact knowledge of the size, contour, and color of the objects that the pilot’s body may have hit is extremely helpful in evaluating the injuries observed in and on the body. The pathologist should confer with pilots, engineers, and other experts who are familiar with the aircraft, parachute, ejection mechanism, and other equipment, to gain firsthand knowledge.
The second step in the investigation is for the pathologist to acquaint himself or herself with all available information relative to the flight: the nature of the accident, severity of damage at the crash site, known factors about the weather, airfield, the health record and past performance of the pilot and his or her condition before and during flight, information regarding the passengers, the nature of any radio contact, and other pertinent information. Similarly, the same factors for the flight attendants must be gathered for analysis later.
The third step in the pathologist’s investigation consists of careful observation and written and photographic records of the position of the body and its relation to the total wreckage (or the parachute and other escape mechanism), and the conditions under which the body was found. The pathologist should examine carefully the pilot’s protective helmet, clothing, shoes, and any other attachments. For flight attendants, the duty locations and seats should be examined with respect to their failure modes. Regarding passengers, examiners should look for extremity fractures that could correlate with seat failures or overhead bin collapse, as well as evidence of inhalational toxins. Examiners should compare where passengers were assigned seats, or actually sat, and their final resting location within the fuselage or outside the aircraft. Using representative yet simple diagrams and simple color-coding schemes, one can store a multitude of details regarding the postcrash events in the field phase of the investigation. In Figures 25-10 and 25-11 some of the survival factors information is encoded visually. In the absence of the pathologist on the crash scene, these items should be left on the body as recovered. No article of clothing, harness, and so on should be cut or removed before inspection by the pathologist. The protective helmet and articles of clothing, shoes, gloves, and so forth, may reveal important information about the crash and may suggest defects in the design of the plane. The soles of the shoes or boots may contain a reversed imprint from the rudder pedals of whatever logo or pattern is on the rudder pedal surface. Cytologic and ultraviolet light studies may offer helpful data.
FIGURE 25-10 Typical on-scene working document for aircraft occupant egress, injury, and death information as part of the field notes of the Survival Factors Group (photo courtesy of Civil Aerospace Medical Institute).
The fourth step performed by the pathologist and his assistants will consist of meticulous examination of the exterior of the body and the viscera, with necessary close-up photographs and radiographs, and removal of properly selected tissue for chemical, toxicologic, and histopathologic examination. Special attention must be directed to the detailed examination of all abrasions, lacerations, and superficial and deep wounds. For example, a single small wound on the lateral or posterior portion of the lower legs may be strong evidence that ejection occurred but that the individual’s feet were not positioned properly at the time. Photographing such wounds will be of great assistance in later correlation of the findings. Specimens of urine, blood, liver, kidney, and brain (unfixed) are necessary for toxicologic analysis for over-the-counter, prescription, or illegal medications and drugs. In recent years, alternative medicine compounds have arisen as another factor to be examined in postmortem testing. For histopathologic examination, tissue sections from all organs—including the skin, bone, middle and inner ears, entire brain, spinal cord, entire heart and aorta, and organs showing significant lesions—should be preserved in 10% neutral formalin. These sections should include not only the diseased or traumatized area of the organ, but also its margin and the adjacent normal area. In cases where a less than complete body is recovered, the examination of the remains should be conducted as conditions permit. It is essential to find as much of the body and internal organs as possible. The condition of the heart, brain, spinal cord, larynx, liver, skeletal muscle, and bone may well explain the cause of the crash.
The fifth stage in the investigation consists of microscopic study of the sections and chemical analysis for poisons. The pathologist must take special notice of the occurrence of vital processes such as vascular dilatation and the cellular exudation of early inflammation in the proximity of burns, contusions, and so forth.
Summarizing the report of the accident and correlating it with the findings of the autopsy complete the final step in the investigation. On scene the factual findings will be captured in a group collection of field notes (human performance, survival factors, etc.), which will be coalesced into group factual reports as further information is collected after the on-scene phase. Eventually the investigating authority will publish a common final report with the facts, findings, probable causes, conclusions, and safety recommendations. The pathologist may participate in the proceedings of the investigating board (24).
Only gold members can continue reading. Log In or Register to continue