Aesthetic Aspects of the Treatment of Breast Cancer
|

The aesthetic impact of all surgical interventions on the breast should be considered prior to the procedure, whether a needle biopsy or mastectomy. Incision placement should allow adequate access and the incision should be placed with consideration of the skin crease lines and how obtrusive the scar may be. Resection of skin or large amounts of breast tissue distorts the breast, particularly if followed by radiotherapy, and the effect of this should be considered. While a mastectomy always has a profound impact on body image, a flat scar without a dog ear of tissue at either end is crucial to allow placement of an external prosthesis and psychological adjustment to the procedure. Incision planning and the use of techniques to avoid unsightly wounds such as fishtailing may assist this.
The increasing awareness of oncoplastic techniques has allowed excision of large amounts of breast tissue without distorting the breast shape. This is performed by volume displacement – mobilization of breast tissue to minimize a defect; volume replacement – filling a defect with tissue from elsewhere (usually the latissimus dorsi muscle); and by surgery on the contralateral, normal breast to maintain symmetry using reduction mammoplasty techniques. One potential problem with oncoplastic procedures is that they tend to be used in young women where the risk of recurrent disease is appreciable and in whom further procedures may therefore be necessary. If a latissimus flap has already been used, then this does limit the techniques available for subsequent breast reconstruction if mastectomy becomes necessary.
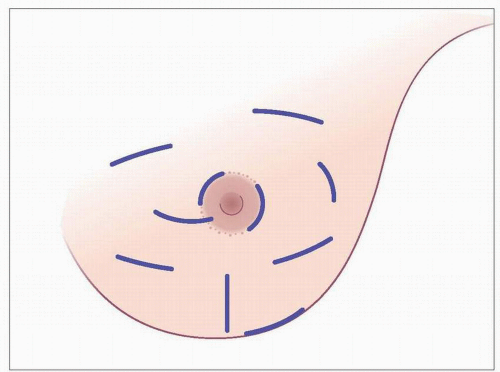 12.1 Potential incisions for excision of breast lesions. The collagen fibres within the skin of the breast are generally arranged circumferentially (Langer’s lines), while the lines of maximum resting skin tension are transverse (lines of Kraissl). Skin incisions in line with both of these heal best. |
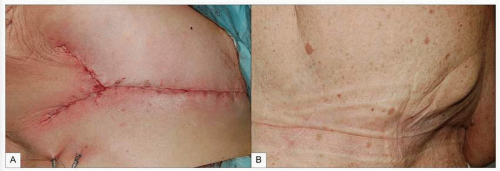 12.2A, B The normal mastectomy incision scar can leave an awkward dog ear in the axilla. Pulling the lateral corner of the wound medially and closing the wound in a Y-shape may help leave a flat scar (fish tail scar). Intraoperative and late results are shown. |
 12.3 Another option for trying to abolish the lateral dog ear following mastectomy is to use a Wise-pattern type incision as used for breast reduction. |
 12.4 A selection of external breast prostheses worn in the bra following mastectomy. Patients are usually discharged home following mastectomy with a soft fabric-covered generic prosthesis. Once the wound has healed, they are formally fitted for a prosthesis of more natural shape, size, and weight to match the remaining breast. |
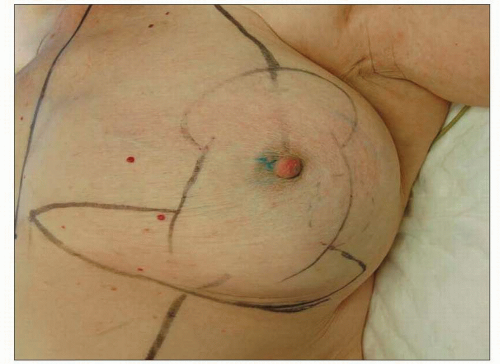 12.5 Surgical treatment of a breast cancer using a reduction mammoplasty. This patient presented with a 4 cm breast cancer in the left lower outer quadrant. Wide excision of the cancer would have resulted in marked distortion of the breast and thus mastectomy would be the normal surgical approach. However, the patient has large breasts and an alternative is to use a breast reduction approach. A large volume of breast tissue including the cancer is removed and the breast reformed as in a breast reduction with a similar procedure performed on the normal right side to maintain symmetry. The site of the cancer is shown with a dotted circle with planned incision lines also marked. |
Breast reconstruction
All women undergoing mastectomy who are fit enough to undergo the procedure should be offered breast reconstruction. It is impossible to replace the breast but various surgical techniques can be used to create a breast mound which provides reasonable symmetry with the normal side when clothed and, ideally, naked. Unless the nipple has been preserved at the initial mastectomy procedure, it will be absent (but it can also be reconstructed). Reconstructed breasts have variable amounts of scarring and numbness. The reconstructed breast will also often not become ptotic with age particularly if an implant-based reconstruction has been used. Breast reconstruction can be performed at the time of mastectomy or at any time after oncological treatment is complete. There is no evidence that immediate reconstruction significantly delays subsequent adjuvant treatment but the adjuvant treatment (particularly radiotherapy) may affect the appearance and texture of the reconstructed breast and so affect selection of the type of reconstruction. It may not be possible to reconstruct a symmetrical breast but the patient may not want a breast of the same dimensions as the original and additional surgery can be performed on the contralateral normal breast either to reduce its size with breast reduction or to increase the size (augmentation) with an implant to achieve symmetry.
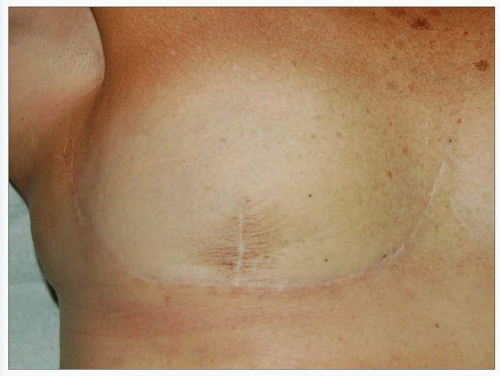
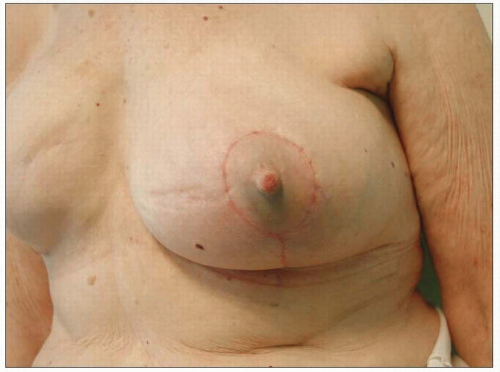 12.6 Postoperative result following reduction mammoplasty for large breast cancer. A good breast shape can be maintained with acceptable scarring. The operative procedure takes longer and surgery on the normal contralateral breast is required. The blue staining on the skin in this case is from the patent blue dye used for sentinel node biopsy. |
There are three commonly used techniques for breast reconstruction with multiple minor variations. These replace the breast volume with either implants or tissue brought from elsewhere or a combination of both. The choice of reconstruction will depend on the circumstances and wishes of the patient following discussion of the risks and expectations of each procedure with the surgeon and breast care nurse.
Expander/implant reconstruction (Figures 12.7, 12.8




Related posts:

Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
