Successful surgical resection offers the only chance for cure in patients with pancreatic cancer. However, pancreatic resection is feasible in less than 20% of the patients. In this review, the current state of surgical management of pancreatic cancer is discussed. The definition of resectability based on cross-sectional imaging and the technical aspects of surgery, including vascular resection and/or reconstruction, management of aberrant vascular anatomy and extent of lymphadenectomy, are appraised. Furthermore, common pancreatic resection-specific postoperative complications and their management are reviewed.
Key points
- •
Despite successful surgical resection, recurrence rates remain high and overall survival is less than 20%.
- •
Advances in cross-sectional imaging and diagnostic modalities such as endoscopic ultrasound have allowed better characterization and selection of patients that will benefit from upfront surgical resection versus neoadjuvant therapy to improve the probability of achieving microscopically negative margins (R0).
- •
Margin-negative resection is possible in the setting of vascular involvement in borderline resectable and selected locally advanced patients after neoadjuvant therapy with vascular resection and/or reconstruction.
- •
Although mortality rates in high-volume centers are low, morbidity rates after resection remain significant, and efforts to minimize these complications are important to allow for the expeditious use of adjuvant therapy.
Introduction
Pancreatic cancer remains one of the most lethal diseases worldwide. Although surgical resection combined with multimodality therapy affords a significant survival advantage in some patients, the vast majority of patients present with locally advanced (LA) or metastatic disease for which palliation is the only option. For those patients who are candidates for resection, surgical options include a pancreaticoduodenectomy (PD), distal or left pancreatectomy (LP), or total pancreatectomy (TP), depending on the location of tumor within the pancreas.
Although surgical resection was initially associated with significant perioperative mortality, advances in surgical technique and perioperative care have reduced the mortality to the low single digits in high-volume centers. In addition, improvements in preoperative imaging modalities have enabled better determination of the extent of disease and have thus allowed for better operative planning and patient selection as well as better standardization of treatment regimens. Nevertheless, perioperative morbidity remains a significant problem and can often result in inadequate administration of appropriate adjuvant therapy. However, even in those patients who undergo successful surgical resection and appropriate adjuvant therapy, 5-year survival rates remain low, ranging from 5% to 15%.
In this review, the current state of surgical management of resectable and borderline-resectable (BR) pancreatic cancer is discussed, focusing on both the technical aspects and the common postoperative complications and their management.
Introduction
Pancreatic cancer remains one of the most lethal diseases worldwide. Although surgical resection combined with multimodality therapy affords a significant survival advantage in some patients, the vast majority of patients present with locally advanced (LA) or metastatic disease for which palliation is the only option. For those patients who are candidates for resection, surgical options include a pancreaticoduodenectomy (PD), distal or left pancreatectomy (LP), or total pancreatectomy (TP), depending on the location of tumor within the pancreas.
Although surgical resection was initially associated with significant perioperative mortality, advances in surgical technique and perioperative care have reduced the mortality to the low single digits in high-volume centers. In addition, improvements in preoperative imaging modalities have enabled better determination of the extent of disease and have thus allowed for better operative planning and patient selection as well as better standardization of treatment regimens. Nevertheless, perioperative morbidity remains a significant problem and can often result in inadequate administration of appropriate adjuvant therapy. However, even in those patients who undergo successful surgical resection and appropriate adjuvant therapy, 5-year survival rates remain low, ranging from 5% to 15%.
In this review, the current state of surgical management of resectable and borderline-resectable (BR) pancreatic cancer is discussed, focusing on both the technical aspects and the common postoperative complications and their management.
Determining resectability
Whether a pancreatic tumor is amenable to surgical intervention is defined by the probability of achieving microscopically negative margins (R0) at the time of resection. Numerous studies have demonstrated a strong correlation between R0 resections and decreased recurrence rates and improved overall survival (OS). Accordingly, margin status remains one of the most important predictors of long-term survival in pancreatic cancer. The status of the resection margin is often cited as a significant predictor of patient outcomes following PD, with the median survival of patients with microscopically positive (R1) resection significantly decreased as compared with those undergoing R0 resection. However, this is not without some controversy, as some studies do not indicate significant differences in survival between these 2 groups when controlled for other prognostic factors. Overall, in patients undergoing PD for resectable disease, there is wide variance in the reported R1 resection rates with those rates varying from 20 to more than 80%. These differences represent differences not only in patient selection and operative technique but also in the identification and analysis of the specimen by pathologists.
Although dependent on what type of resection being performed, margins during pancreatic resection typically include the following:
- •
Transection margins
- ○
Pancreatic neck margin
- ○
Common bile duct (CBD)/hepatic duct (CHD) margin
- ○
Distal stomach/proximal duodenum
- ○
- •
Circumferential margins
- ○
Anterior pancreatic margin
- ○
Posterior pancreatic margin
- ○
Superior mesenteric artery (SMA) margin
- ○
Superior mesenteric vein (SMV) margin
- ○
Radial CBD/CHD margin
- ○
Importantly, the transection margins can generally be extended if intraoperative analysis (usually by frozen section) suggests disease involvement. Circumferential margins are less clearly defined, and extending these margins is more difficult.
Unfortunately, there are no clear consensus guidelines addressing the pathologic analysis of PD specimens, including the number or types of margins, inking practices, or even diagnostic criteria for positivity. For example, in European studies, tumor found within 1 mm of the resection is defined as R1 resection, whereas in the United States, tumor must be present at the margin. Moreover, the inflammation, atrophy, and fibrosis associated with pancreatic cancer, particularly in the setting of prior pancreatitis or neoadjuvant chemoradiation therapy, make the analyses of margins more difficult. Careful multicolor inking of the specimen with extensive sampling and thin axial slices as well as adoption of the European definition of R1 resection has been show to lead to more accurate R1 margin rates. In fact, when careful pathologic analysis is performed, R1 resection rates tend to be higher and the discrepancy between the survival of patients undergoing R0 and R1 resections are more pronounced. Current College of American Pathologists guidelines are vague and recommend “inking the posterior surface of the pancreas and submission of sections through the tumor at its closest approach to this surface as well as the retroperitoneal (uncinate) margin.”
In determining resectability, the main barrier to achieving R0 resection remains the relationship of the tumor to the mesenteric vasculature. The goal of preoperative staging and imaging, therefore, is not only to evaluate for metastatic disease but also to delineate the relationship of the relevant vasculature structures to the tumor, including the common hepatic artery (CHA), gastroduodenal artery (GDA), SMA, celiac axis, SMV, portal vein (PV), and the SMV-PV confluence. Preoperative staging and imaging enable the patient’s tumor to be appropriated into 1 of 4 categories: resectable, BR, LA, or metastatic. One of the major obstacles in determining resectability of pancreas cancer has been the lack of a unified definition of these categories. Several institutions and agencies have published definitions; however, significant variation persists.
Resectable Disease
In general, upfront resectable disease is defined as
- •
Tumor without contact with the celiac artery (CA), hepatic artery (HA), SMA, or SMV, suggesting a high likelihood that margin-negative resection can be achieved without preoperative therapy ( Fig. 1 A )
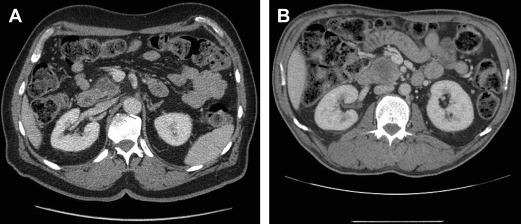
Fig. 1
( A ) Cross-sectional imaging of a resectable pancreatic adenocarcinoma with preservation of a fat plane between the tumor and the SMV and SMA. ( B ) Resectable pancreatic adenocarcinoma with less than 180° involvement of the SMV but with a preserved fat plane between the tumor and SMA.
With improvements in surgical technique and vascular resection, some groups also include tumors with limited involvement of the SMV-PV confluence in which an R0 resection is still possible, albeit with vascular resection and reconstruction in the resectable category ( Fig. 1 B). For example, the MD Anderson Cancer Center (MDACC) definition deems tumors resectable if there is abutment of the SMV-PV with patent vessels. The National Cancer Center Network (NCCN) also allows for 180° contact or less of the SMV-PV but only in the absence of any vein contour irregularity.
Locally Advanced Disease
The definition of LA disease also varies, although in general, LA characterizes patients in whom the likelihood of attempting to resect the tumor even after treatment with systemic or locoregional therapy to allow a margin-negative resection is essentially minimal. Although several varying definitions exist, essentially tumors with extensive vascular involvement especially arterial involvement are deemed LA ( Fig. 2 , Table 1 ).

| Vessel Involved | MDACC | AHPBA/SSO/SSAT | NCCN/ISGPS |
|---|---|---|---|
| SMA | Encasement | Encasement | Contact >180° or contact with first jejunal SMA branch |
| CHA | Encasement—unable to reconstruct | Encasement with extension to CA | Contact with extension to CA or bifurcation |
| Celiac axis | Encasement | Abutment or encasement | Contact >180° |
| SMV-PV confluence | Occluded—unable to reconstruct | Occluded—unable to reconstruct | Unable to reconstruct |
Borderline Resectable Disease
The original term marginally resectable was coined to identify patients at high risk of a macroscopically positive (R2) resection with upfront surgery. The term BR pancreas cancer was subsequently adopted by the NCCN in 2006 to describe patients who might benefit from neoadjuvant therapy in order to reduce the likelihood of margin positivity. Unfortunately, what defines BR disease remains an area of significant controversy.
Over the past decade, several different classification schemes have been published to describe which patients are considered BR pancreatic cancer, including consensus statements and guidelines from the NCCN; the International Study Group of Pancreatic Surgery (ISGPS); MDACC; Americas Hepato-Pancreato-Biliary Association/Society of Surgical Oncology (AHPBA/SSO); the Society for Surgery of the Alimentary Tract (SSAT); and the Moffitt Cancer Center ( Fig. 3 , Table 2 ).

| Vessel Involved | MDACC | AHPBA/SSO/SSAT | NCCN/ISGPS | Moffitt |
|---|---|---|---|---|
| SMA | Abutment | Abutment | Abutment | Abutment |
| CHA | Abutment or short segment encasement | Abutment or short segment encasement | Abutment without extension to celiac or HA bifurcation | Abutment or short segment encasement |
| Celiac axis | Abutment | No abutment or encasement | No contact | Not specified |
| SMV-PV confluence | Short-segment occlusion amenable to reconstruction | Abutment, encasement, or occlusion amenable to reconstruction | Abutment or encasement amenable to reconstruction | Abutment or encasement amenable to resection |
Despite what would seem to be rather objective criteria, all of these definitions are somewhat subjective and are continually evolving. In the recent Alliance Trial (A021101), a multi-institutional single-armed trial designed to evaluate toxicity and feasibility of neoadjuvant chemotherapy and chemoradiation for BR pancreatic cancer, for example, the investigators advocated for an easily reproducible definition based on more objective data obtained from computed tomographic (CT) imaging, avoiding subjective terms like abutment or encasement. The Alliance definition consisted of the following: (1) an interface between the tumor and SMV-PV 180° or greater of the vein wall circumference; (2) short-segment occlusion of the SMV-PV with normal vein above and below the obstruction amenable to resection and reconstruction; (3) short-segment interface of any degree between tumor and HA with normal artery proximal and distal to the interface amenable to arterial resection and reconstruction; and (4) interface between the SMA and CA measuring less than 180° of the circumference of the artery.
Diagnostic workup
Imaging Modalities
Imaging modalities including CT, MRI, and endoscopic ultrasound (EUS) are the mainstay in the diagnosis and staging of pancreatic cancer, and advances in these techniques have dramatically improved the preoperative determination of resectability for pancreatic cancer. Specifically, the development of multi-detector-row CT allows for high-resolution scan as well as 3-dimensional (3D) reconstructions; this, in addition to a “pancreas protocol CT,” which includes 3 phases (arterial phase, pancreatic parenchymal phase, and venous washout phase), has given physicians the ability to analyze the relationship of the pancreatic tumor to important vascular structures discussed above. CT is also effective in detecting lymphadenopathy and peritoneal and liver metastases. Enhanced MRI (with gadolinium or pancreatic tumor, excluding mangafodipir trisodium) is also effective in detecting local extension and vascular involvement. It is often superior to CT in detecting small liver lesions. Magnetic resonance cholangiopancreatography has the added benefit of noninvasively evaluating biliary and pancreatic ducts. Finally, EUS is highly sensitive for the detection of small tumors, surpassing both CT and MRI in this regard, as well as lymph node (LN) metastases and vascular invasion. In addition, EUS provides the safest avenue for pathologic confirmation of disease, which is crucial for those patients undergoing neoadjuvant therapy.
The Role for Diagnostic Laparoscopy
Although CT and MRI are highly sensitive for detection of LA as well as distant metastatic disease, small liver metastases and peritoneal disease may be undetectable even with high-quality axial imaging. As a result, many surgeons advocate the use of diagnostic laparoscopy before attempted resection, especially among patients with findings suspicious for advanced disease on imaging, such as ascites, indeterminate liver lesions, or peritoneal or omental thickening. Staging laparoscopy is not as useful for determining resectability of LA disease because tumor involvement of the vasculature, specifically the SMA, which is not easily detected by laparoscopy.
A Cochrane database review of the use of diagnostic laparoscopy demonstrated a decreased laparotomy and aborted resection rate from 40% with CT alone to 17% with CT combined with diagnostic laparoscopy. If metastatic disease is detected, staging laparoscopy not only decreases hospital length of stay but also allows patients to initiate chemotherapy significantly earlier than those undergoing exploratory laparotomy.
An adjunct to laparoscopy includes peritoneal washings. Notably, positive peritoneal cytology occurs in 7% to 30% of potentially resectable cases, and those patients have similar outcomes to those with metastatic tumor burden; thus, they are generally not considered candidates for radical resection. By NCCN standards, positive washings are considered stage IV disease. The use of peritoneal washings for patients with pancreatic cancer, however, is not universally used.
Vascular resection during pancreaticoduodenectomy
Although historically abandoned due to poor outcomes, vascular resection, particularly venous resection, has now gained widespread acceptance in the resection of pancreatic cancer in selected patients. There is near universal agreement, however, that aggressive vascular resections for patients with BR disease should only be performed in patients with favorable tumor biology who have received neoadjuvant therapy before resection and by surgeons experienced in these procedures.
Ideally, the need for vascular resection is determined preoperatively, although this is not always possible. Signs of vascular involvement on cross-sectional imaging include proximity of tumor, loss of the fat plane or interface between a given vessel and tumor, and narrowing or impingement of venous structures (see Fig. 1 ). Narrowing of vein is highly specific, but not sensitive, for tumor involvement. Arterial involvement is more easily defined by CT preoperatively given the nerve plexus and fat plane normally surrounding an artery (see Fig. 2 ).
However, more than 40% of tumors ultimately requiring vascular resection and reconstruction did not clearly demonstrate findings suggestive of vascular resection on preoperative imaging, again underscoring the importance of centralization of pancreatic cancer care to high-volume centers in which surgeons are experienced and facile with vascular reconstruction or to medium volume centers at which a vascular surgeon is available to assist with resection and reconstruction. Importantly, one study indicated that the cross-sectional imaging before neoadjuvant therapy was more predictive of vascular involvement than imaging performed after completion of preoperative therapy. The investigators found initial imaging to be 98% predictive of vascular involvement compared with only 25% after neoadjuvant therapy.
Venous Resections
Resection of the SMV, PV, or SMV-PV confluence is not uncommon at high-volume centers. Reports indicate that an average of 30% (7%–80%) of PDs performed at major medical centers now include venous resection and reconstruction. Perioperative morbidity and mortality associated with venous resection and reconstruction are similar to PDs performed without any venous construction, with short-term mortality ranging from 4% to 12% and complications ranging from 17% to 100%.
Venous resection and reconstruction can vary in extent, including the following:
- •
Partial lateral venorrhaphy with transverse closure
- •
Resection with vein patch
- •
Interposition graft with either autologous or prosthetic vein graft
Patch reconstruction with autologous vein is standard practice; however, both cadaveric allografts and xenografts (porcine peritoneum, bovine pericardium) have also been used. The autologous vein of choice for interposition grafts is the internal jugular vein or greater saphenous vein, but other conduits, including the superficial femoral, left renal, and inferior mesenteric veins (IMVs), have also been used. The risk of prosthetic graft in a potentially contaminated operative field with risk of pancreatic fistula is significant; thus, prosthetic grafts are not recommended but are sometimes required if suitable autologous vein is not available. Notably, up to 5- to 7-cm gaps can be primarily anastomosed with division of splenic vein (SV), mobilization of the right colon, hepatic flexure, and root of the mesentery and full mobilization of the liver, often obviating interposition graft.
Splenic Vein Ligation and Sinistral Hypertension
As noted, division of the SV to allow for additional mobilization enabling an end-to-end anastomosis and eliminating need for interposition graft is commonly practiced. In addition, when tumor involvement includes the area of confluence of SV and SMV, the SV is often ligated and divided. However, division of the SV has the theoretic risk of sinistral or left-sided portal hypertension. Some studies have demonstrated increased frequency of sinistral hypertension as defined by an increase in spleen volume or decrease in platelet count. In addition, there are case reports of hypertensive gastropathy with gastric varices and gastrointestinal (GI) bleed following SV ligation during PD. Any theoretic risk of SV thrombosis and sinistral hypertension can be avoided by preservation of not only the short gastric vessels but also the SV-IMV confluence, both of which would allow for decompression of the SV to the systemic circulation. In addition, reanastomosis in an end-to-end fashion of SV to IMV, use of an interposition graft, or even a distal splenorenal shunt, mesocaval shunt, or IMV to right gastroepiploic vein anastomosis may be performed.
The incidence and clinical significance of this theoretic complication have been called into question by several studies. In one study, only a very limited number of patients in whom the SV had been ligated actually developed clinically significant splenomegaly. The reasons for this are likely many. For one, survival following PD may not be long enough for this process to manifest itself. In addition, following ligation of the SV, venous blood can re-enter the systemic circulation via the esophageal veins or right colic tributaries. Finally, tumor involvement of the SV or confluence can cause relative stenosis, and collateral vessels may already be well developed at the time of PD.
Arterial Resections
Although venous resection is not uncommon, consensus guidelines still consider extensive tumor involvement of major arteries (SMA, celiac, and common hepatic arteries) to be unresectable. In a recent meta-analysis, patients undergoing arterial reconstruction were associated with increased operative times, higher morbidity rate, including vascular and nonvascular complications, and a higher rate of reoperation, as well as an increased mortality rate. Patients who underwent combined venous and arterial resection had worse outcomes when compared with patients undergoing venous reconstruction alone. In addition, the 1-, 3-, and 5-year survival rates of PD with arterial resection were worse than PD alone and to PD with venous reconstruction. It should be noted, however, that this meta-analysis included a heterogeneous patient population over an extended time period (1977–2010), during which significant improvements in patient outcomes as well as advancements in neoadjuvant therapy regimens took place.
At the current time, greater than 180° abutment, or encasement of the SMA, is considered a contraindication to resection. There has, however, been limited experience but acceptable outcomes achieved in young, otherwise healthy individuals who underwent extended resection for LA disease involving the CHA or celiac axes after completion of neoadjuvant chemotherapy at high-volume centers. In nearly all patients who require arterial resections, venous resections are also required, further increasing the complexity and potential morbidity of the resection.
Postoperative Anticoagulation
Although the risk of mesenteric or PV thrombosis may be increased in patients undergoing resection for malignancy, it appears to be particularly increased when vascular reconstruction is performed. It is important that the anastomoses or graft is not twisted or kinked in any way, and all venous anastomoses should allow for dilation and avoid a “waist” at the suture line once normal venous flow is re-established.
A recent review article in 2014 found a rate of thrombosis of 25% with reconstruction. Thrombosis can range from partial occlusion of the SMV or a lesser tributary to the more feared complication of early or late PV thrombosis. The area and extent of resection and reconstruction almost certainly influence venous thrombosis rates. Rates of thrombosis with polytetrafluoroethylene grafts are consistently higher than interposition grafts using autologous vein; most studies report patency rates of approximately 90% for autologous vein conduit.
Patients may be asymptomatic or, rarely, may develop severe peritonitis secondary to acute mesenteric ischemia. Early PV thrombosis is associated with a 30% to 40% mortality rate. Although early thrombosis is deadly, patients with delayed PV thrombosis following PD with vascular reconstruction have survival rates greater than those without thrombosis presumably because of interval development of collateral flow.
Intraoperative systemic anticoagulation during reconstruction is not routinely used. Some surgeons advocate its routine use, whereas others advocate its use when the SMA is formally clamped for an extended period; there are no data to support or refute its use. Data supporting the use of postoperative anticoagulation for patients undergoing vascular reconstruction during PD likewise are sparse. Most protocols are based on surgeon preference. A recent review article in 2014 summarized the available data; however, given the wide variation in practice in the primary articles (heparin and warfarin vs aspirin), no firm conclusions could be drawn. A more guided prospective multi-institutional research trial would be necessary to define best practice standards with regards to anticoagulation for venous reconstruction. Current practice at the authors’ institution involves the use of low-dose aspirin postoperatively for all PDs requiring vascular reconstruction.
Aberrant vascular anatomy and celiac stenosis
As many as 20% to 50% of patients exhibit aberrant vascular anatomy. The variants most critical for the surgeon during PD include an accessory or replaced right hepatic artery (RRHA) and replaced common hepatic artery (RCHA) because they typically course through an area predisposed to tumor involvement. Although these aberrancies may add to the complexity of the operation, it is not clear whether these variants affect resectability. Although traditionally these abnormalities may have been discovered in the operating room, modern multiphase imaging techniques nearly always identify these abnormalities preoperatively and allow for proper operative planning.
Replaced Right and Common Hepatic Arteries
The most common variant overall is an RRHA, which branches from the SMA, and is seen in 11% to 20% of individuals. It typically courses behind or through the pancreatic head, predisposing it to tumor involvement especially with posteriorly located malignancies. Fortunately, an RRHA can often be preserved with careful dissection even with tumor nearby. If division is required, the primary concern is preservation of blood flow to the CBD, which could lead to failure of the bilioenteric anastomosis or delayed anastomotic stenosis. Given this, some argue that it is important to attempt to reconstruct if the replaced RHA must be sacrificed (either primarily or using an autologous vein graft), although this may be technically difficult given its small diameter. A second anatomic variant of concern to the surgeon performing PD is the rarer RCHA, in which the CHA originates from the SMA. Fortunately, this variant occurs only in 0.4% to 4.5% of population. If the replaced CHA has an intrapancreatic course, reconstruction is usually necessary.
Celiac Artery Stenosis
Celiac artery stenosis is most often secondary to intrinsic disease (plaque) or extrinsic forces secondary to either nodal disease burden, median arcuate ligament syndrome, or a tumor-associated fibroinflammatory process. Celiac stenosis is encountered in up to 5% of all pancreaticoduodenectomies. Most patients are asymptomatic due to the propensity for extensive collateralization; the CHA receives retrograde flow via the GDA or dorsal pancreatic artery coming off the SMA, or via the Arc of Buhler, which is a direct connection between SMA and CHA. Elimination of collateral flow by division of the GDA during PD in the setting of celiac stenosis has theoretic and observed implications for compromised flow to liver, stomach, and spleen.
Preoperatively, CT imaging has low sensitivity for detecting clinically significant celiac stenosis but significant collateralization or an unusually large GDA raises suspicion. Given this low sensitivity, it should be routine practice during PD to assess flow within the HA by temporarily occluding flow from the GDA before division. Significant stenosis from atherosclerosis that is identified preoperatively can be managed with angioplasty and stent, but the long-term outcome is not clear. Intraoperatively, if blood flow in the proper HA becomes significantly reduced following ligation of the GDA, it is recommended that restoration of flow be performed. In cases with eccentric compression, division of the median arcuate ligament is successful in up to 70% of cases. If that is not successful or if reduced blood flow is due to other reasons, an autologous graft from the aorta to the proper HA is recommended.
Lymphadenectomy in pancreatic cancer
A large proportion of pancreatectomy specimens contain positive nodes, ranging from 50% to 80%. Lymphatic spread is thought to begin with peripancreatic nodes either by direct invasion or via lymphatic channels, then spreading to SMA and CHA nodes, and finally, to para-aortic nodes.
LN involvement is a significant negative prognostic factor. The 5-year actuarial survival of patients with node positive disease is 5%, as compared with 10% survival among patients with node-negative disease. Local recurrence rates are also significantly higher in those with LN-positive disease. Survival is increased dramatically with N0 resection, and, within N0 resections, there is increased survival with increased nodal sampling. In addition, for N1 disease, the LN ratio (positive LN/resected LN) is critical, with ratios of 0 to 0.2 having more favorable outcomes than 0.2 to 0.4, underscoring the responsibility of both surgeon and pathologist to provide an adequate nodal assessment at the time of PD. At least 12 to 15 nodes are recommended for adequate analysis. Similar to pathologic analysis of specimen margins, however, the quality of LN evaluation within a given surgical specimen varies significantly.
It is not known which groups of nodes offer the most prognostic impact, or whether nodal invasion of peripancreatic LNs, likely by direct invasion, has the same prognostic implication as true lymphatic dissemination into nodal groups further from the primary mass. In one study, peripancreatic nodal invasion only had survival rates similar to those without nodal invasion, whereas, in others, direct invasion had similar prognostic implications as true lymphatic spread. In general, however, patients with involvement of a single nodal group have better outcomes than involvement of multiple nodal groups.
Extended Lymphadenectomy
Although the prognostic impact of overt nodal spread is rarely disputed, there was, for some time, significant debate as to whether aggressive nodal dissection at the time of PD to attain locoregional control of disease truly affected outcomes.
The need for definition of a standard nodal dissection was addressed at the 2013 ISGPS consensus meeting. The standard lymphadenectomy for PD should include the following:
- •
The peripancreatic tissue to the right of SMA and proper HA—specifically nodal stations 5, 6, 8a (proper HA), 12b, 12c, 13a, 13b (posterior surface), 14a (right lateral SMA), 14b (right lateral SMA), 17a, 17b (anterior surface) as defined by the Japanese Pancreas Society
Anything beyond this is considered an extended lymphadenectomy.
Several meta-analyses have revealed no improvement in survival with extended lymphadenectomy, as extraregional LN involvement should be considered metastatic disease. In addition, more extensive dissections are associated with higher rates of postoperative complications, including delayed gastric emptying (DGE), increased weight loss, and diarrhea thought to be secondary to autonomic disruption.
Related posts:
 Molecular and Genetic Basis of Pancreatic Carcinogenesis
Molecular and Genetic Basis of Pancreatic Carcinogenesis
 Role of Endoscopic Ultrasonography and Endoscopic Retrograde Cholangiopancreatography in the Clinical Assessment of Pancreatic Neoplasms
Role of Endoscopic Ultrasonography and Endoscopic Retrograde Cholangiopancreatography in the Clinical Assessment of Pancreatic Neoplasms
 Minimally Invasive Approaches to Pancreatic Surgery
Clinical Presentation and Diagnosis of Pancreatic Neuroendocrine Tumors
State-of-the-art Imaging of Pancreatic Neuroendocrine Tumors
Surgical Management of Pancreatic Neuroendocrine Tumors
Minimally Invasive Approaches to Pancreatic Surgery
Clinical Presentation and Diagnosis of Pancreatic Neuroendocrine Tumors
State-of-the-art Imaging of Pancreatic Neuroendocrine Tumors
Surgical Management of Pancreatic Neuroendocrine Tumors
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


