Fig. 16.1
Axial apparent diffusion coefficient map of a corresponding patient demonstrating prostate tumor at left peripheral zone
Conventional 18-fluorodeoxyglucose (FDG) PET-CT has been widely used for various tumors [15–19]; however, its role in prostate cancer is limited. Choline PET and 18F-fluciclovine PET are other nuclear imaging modalities for prostate cancer [20]. The use of choline PET remains unclear for its value in initial staging. In the restaging phase, the detection rate of choline PET varies between 21% and 82%, which is dependent on site of recurrence and PSA levels [21]. A systematic review showed that the sensitivity and specificity of 18F-fluciclovine PET for prostate cancer was 87% and 66% [20]. There is an increasing investigation about specific markers related to prostate cancer. Prostate-specific membrane antigen (PSMA) is overexpressed in prostate cancer cell membranes [22]. The PSMA-PET is a highly selective imaging tool for detecting the primary, involved lymph nodes and distant metastasis in prostate cancer patients (Fig. 16.2). Also the importance of PSMA PET in identification of both local and distant recurrences was shown in many trials with a detection rate for recurrent disease of approximately 85–90% [23, 24]. The detection rate is correlated with PSA value and decreasing to 58% between PSA values of 0.2–0.5 ng/ml [24]. Furthermore, PSMA-PET is useful in demonstrating IPL, for further dose escalation during prostate RT (Fig. 16.3).

Fig. 16.2
68 Ga-PSMA ligand positron emission tomography/computed tomography images of a representative prostate cancer patient. (a) PSMA-PET -CT image, demonstrating increased uptake in the pelvic and para-aortic lymphatics (arrows). (b) The co-registered images of PET and CT, demonstrating increased Ga-PSMA uptake in the para-aortic lymphatics and (c) in the prostate
Fig. 16.3
68 Ga-PSMA ligand positron emission tomography/computed tomography images demonstrating intraprostatic lesion (light yellow area) in three different representative prostate cancer patients
16.2 New Radiotherapy Delivery Approaches
Historically, the prostate was treated with four static radiation fields designed based on anatomic landmarks. However, with this technique, it is difficult to get idea about the target volume doses and also surrounding organs. As a consequence, geographic misses may be seen more than expected, and it is difficult to know about the toxicities. With the use of a 3D conformal RT (3DCRT) technique, the dose escalation above 70 Gy resulted in a modest increase in rectal and bladder toxicity. With advancements in imaging, more focal three-dimensional treatment plans were developed to target the prostate and seminal vesicles only (Fig. 16.4). Further advances in radiation delivery techniques such as IMRT and volumetric modulated arc therapy (VMAT ) led to greater sparing of adjacent normal tissue to reduce toxicity. Techniques such as VMAT and IMRT are able to generate conformal isodoses, which significantly reduce the OAR doses and normal tissue toxicity [25]. Although IMRT is a commonly used method to treat prostate cancer, the potential downsides of IMRT include increased RT delivery time, resulting in a greater integral body dose, which might increase the risk of secondary cancer development [26].
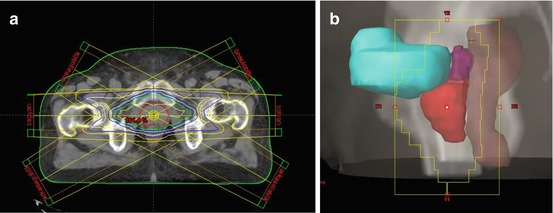
Fig. 16.4
(a) Dose distributions of a seven-field coplanar three-dimensional conformal radiotherapy plan. (b) Beam’s eye view of lateral irradiation field demonstrating prostate and seminal vesicles (red), rectum (brown), and bladder (magenta)
VMAT is an innovative form of IMRT optimization that allows the radiation dose to be efficiently delivered using a dynamic modulated arc. The VMAT simultaneously coordinates gantry rotation, multi-leaf collimator (MLC) motion, and dose-rate modulation, facilitating highly conformal treatment with better normal tissue sparing [27]. Compared with IMRT, the potential advantages of VMAT include a large reduction in monitor units (MU) required to deliver a given fraction size and a concomitant reduction in treatment time (Figs. 16.5 and 16.6). Helical tomotherapy (HT) is an arc-based application of IMRT that uses a fan beam of radiation in conjunction with binary MLC. The gantry rotates at a constant speed, while the binary MLC leaves open 51 times per rotation and close entirely between projections. This rotational treatment modality can establish target dose conformity and OAR dose reduction (Fig. 16.7). Several recent studies have evaluated the use of VMAT delivery methods in prostate cancer (Table 16.1) [28–38].

Fig. 16.5
Representative axial computed tomography slices showing 50% of prescribed dose distributions for (a) 6 MV, (b) 10 MV, and (c) 15 MV energy IMRT plans and (d) 6 MV, (e) 10 MV, and (f) 15 MV energy VMAT plans. Blue area represents 50%, red area represents 95%, and yellow-orange area represents 50–95% of prescribed dose
Fig. 16.6
Representative axial computed tomography slices showing 90% of prescribed dose distributions for (a) 6 MV, (b) 10 MV, and (c) 15 MV energy IMRT plans and (d) 6 MV, (e) 10 MV, and (f) 15 MV energy VMAT plans. Yellow area represents 95%, and red area represents hot spots within the target volume
Fig. 16.7
Helical tomotherapy version HDA used for external beam radiotherapy
Table 16.1
Published studies comparing VMAT and IMRT plans for prostate ± seminal vesicle irradiation
Author (year) | Patient no | TPS | RT dose (Gy) | IMRT beam no | VMAT arc no | IMRT MU/VMAT MU |
|---|---|---|---|---|---|---|
Palma et al. (2008) | 10 | Eclipse/Eclipse | 2/74 | 5 | 1/358° | 1.73 |
Wolff et al. (2009) | 9 | Hyperion/ERGO++ | 2/76 | 7 | 1/360° 1/360° + 2/100° | 1.41 1.47 |
Zhang et al. (2010) | 11 | MSKCC/MSKCC | 1.8/86.4 | 5 | 1/360° | 2.22 |
Rao et al. (2010) | 6 | Pinnacle/Pinnacle SmartArc | 2/78 | 7 | 1/356° | 1.16 |
Sale et al. (2011) | 8 | Eclipse/Eclipse | 1.8/75.6 | 5 | 1/360° 2/360° | |
Tsai et al. (2011) | 12 | Pinnacle/ERGO++ | 2/78 | 5 | 1/360° | 1.08 |
Hardcastle et al. (2011) | 10 | Pinnacle/Pinnacle SmartArc | 2/78 | 7 | 1/360° | 1.23 |
Sze et al. (2012) | 14 | Eclipse/Eclipse | 2/76 | 7 | 1/360° 2/360° | 1.48 1.23 |
Fontenot et al. (2012) | 5 | Pinnacle/Pinnacle SmartArc | 7 | 1/350° | 1.25 | |
Onal et al. (2014) | 12 | Monaco/Monaco | 2/78 | 7 | 1/360° | 1.10 |
Image guidance is essential for delivering the high radiation doses to the prostate accurately. The prostate is a mobile organ influenced by bladder and rectal filling. The position of these structures as defined on the planning CT can vary during and between fractions. Delivery of highly conformal treatments with steep dose gradients demands confidence in localization of the target because motion can lead to geographic miss, underdosing of the tumor, and/or unwanted overdosing of organs at risk. Dedicated CBCT equipment can acquire a 3D CT image in real time in the treatment position just before treatment (Fig. 16.8). Resolution is not of diagnostic quality but enables visualization of soft tissues (prostate, bladder, and rectum) so that table shifts can be made if needed. CBCT can be used in conjunction with fiducial seeds. However, the implantation of fiducial markers is an invasive procedure with the potential for discomfort, bleeding, and infection. Furthermore, fiducial markers provide little information on deformation of the target, localization of the seminal vesicles, or alteration in the neighboring normal tissue and may cause deformation of the prostate gland after implantation. Although fiducial marker implantation for image-guided RT in prostate cancer allows the localization of the prostate during treatment, this application may cause some complications and dosimetric uncertainties. Therefore, alternative noninvasive methods of CBCT should be considered for IGRT of prostate cancer patients [39].
Fig. 16.8
Registration of cone beam CT images and reference CT images. After corrections according to prostate at lateral, superoinferior, and anteroposterior directions, the treatment was delivered with less setup errors
16.3 Radiotherapy Dose Escalation
External beam radiotherapy (EBRT) focusing on intensity-modulated RT (IMRT ) and image-guided RT (IMRT), hypofractionation and stereotactic body RT (SBRT), high-dose rate (HDR) brachytherapy, proton beam RT (PBRT), and ablative therapies such as cryoablation, high-intensity focused ultrasound (HIFU), and radiofrequency ablation (RFA) are therapeutic modalities that have been investigated in patients with PC in an attempt to reduce toxicity while improving cancer control. These treatment modalities could be used as monotherapy, whole prostate, or IPL boost.
A 3 mm thickness planning CT should cover the whole pelvis for RT planning. Patients need to be asked to have a comfortably full bladder and an empty rectum [40]. If MRI or PET fusion is planned to fuse with planning CT, these imaging modalities should be obtained in closest possible condition. In addition to that, in patients planning to receive androgen blockade, imaging should be preferred before the initiation of hormonal therapy [31]. Gross tumor volume (GTV), clinical tumor volume (CTV), and planning tumor volume (PTV) are basically defined in the International Commission of Radiation Units and Measurements (ICRU) [41]. CTV is based on clinical or pathological staging, while appropriate PTV margin is based on the RT technique and image guidance in the oncological center. The rectum, sigmoid colon, small bowels, bladder, and femoral heads are recommended to delineate as OAR. The rectum needs to be delineated from the anal verge to the rectosigmoidal junction. Femoral heads need to be delineated to the level of ischial tuberosities.
Dose escalation for prostate cancer causes improved biochemical control and reduced distant metastasis [2]. However, local failure still occurs in one-third of patients after 78 Gy ERT, and the original IPL is the most frequent location of relapse [42]. Therefore, selectively boosting radiation to these lesions to a very high dose has been hypothesized to be a more effective method to improve the therapeutic ratio than a homogeneous, but more modest, dose escalation to the entire prostate [43]. Randomized trials have shown a gain in BPFS using dose escalation for PC [1, 2]. However, isolated local failure is still reported in nearly one-third of patients, even with higher RT doses [2]. Local recurrence is of clinical importance because a relationship has been suggested between local control, distant metastasis, and survival [44]. Also, it has been demonstrated that local failure mainly originates at IPL. This could be a result of intrinsic resistance of radioresistant tumor clones [42]. So, delivering higher doses to IPL using SIB technique may potentially increase local control and treatment outcomes. The SIB technique can be safely performed by static IMRT , VMAT, or HT (Fig. 16.9). With VMAT plan (Fig. 16.10) and HT plan (Fig. 16.11), a homogeneous dose distribution was observed in target volumes with better sparing of the surrounding organs.
Fig. 16.9
The dose distributions of prostate irradiation and simultaneous integrated boost to intraprostatic lesion in (a) static IMRT plan, (b) VMAT plan, and (c) helical tomotherapy plan
Fig. 16.10
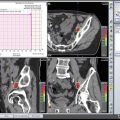
The intraprostatic lesion demonstrated in (a) diffusion-weighted MRI and (b) 68 Ga-PSMA-PET /CT. (c) The dose distribution of prostate (green-yellow area) and intraprostatic lesions (red area) obtained from VMAT plan
Fig. 16.11
The intraprostatic lesion demonstrated in (a) diffusion-weighted MRI. (b–c) The dose distribution of prostate (blue area) and intraprostatic lesions (red area) together with pelvic lymphatics (pink area) obtained from helical tomotherapy plan
There are several studies investigating SIB boost to IPL/whole gland in treatment of PC [12, 32, 45–47] (Table 16.2). A boost to the IPL has been found to be effective and safe [48]. The reported BRFS and DFS rates were 78–92% and 90–100%, respectively [48]. Although SIB to IPL is not a standard approach, several ongoing studies will evaluate whether this approach is effective in local tumor control or not.
Table 16.2
Published studies demonstrating the feasibility of simultaneous integrated boost intraprostatic lesion during prostate radiotherapy
Author (year) | Patient no | Imaging | RT technique/dose | Toxicity |
|---|---|---|---|---|
De Meerleer et al. (2005) | 15 | MRI | Step-shoot IMRT Prostate + 7–10 mm 74 Gy IPL + 0 mm 80 Gy | Acute GI Gr II 3/15 Acute GU Gr III 1/15 Acute GU Gr II 6/15 |
Singh et al. (2007) | 3 | MRI + fiducial | Step-shoot IMRT Prostate + 7–10 mm 75.6 Gy IPL + 3 mm 94.5 Gy | Acute Gr I 1/3 Acute GU 2/3 |
Fonteyne et al. (2008) | 118 (boost) 112 (no boost) | MRI | Step-shoot IMRT Prostate + 8 mm 78 Gy IPL + 4 mm 80 Gy | No increase in toxicity with SIB plan |
Miralbell et al. (2010) | 50 | MRI | Prostate 64–64.4 Gy Hypofractionated boost 5–8 Gy | Late GI Gr II 10% Late GI Gr III 10% Late GU Gr II 12% |
Ippolito et al. (2012) | 40 | MRI | Step-shoot IMRT Prostate + 10 mm 72 Gy IPL + 5 mm 80 Gy | Late GI Gr II 5% Late GI Gr III 2.5% Late GU Gr II 5% |
Wong et al. (2011) | Total 71 SIB 14 | Indium-111-capromad | Step-shoot IMRT Prostate + 4–8 mm 76 Gy IPL + 4 mm 80 Gy | Late GI Gr II 21% Late GU Gr II 39% Late GU Gr III 4% |
Pinkawa et al. (2012) | Total 67 SIB 46 | 18F-choline PET | Step-shoot IMRT Prostate + 6 mm 75.6 Gy IPL + 0 mm 80 Gy | No increase in toxicity with SIB plan |
Aluwini et al. (2013) | 50 14 IPL (+) | MRI + fiducial | Prostate + 3 mm 38Gy/4 fx (daily) IPL 44Gy/4fx | Late GI Gr II 3% Late GU Gr II 10% Late GU Gr III 6% |
Onal et al. (2016) | 173 | MRI | Dynamic IMRT /VMAT Prostate + 5–8 mm 78 Gy IPL + 4 mm 86 Gy | Late GI Gr II 4% Late GU Gr II 3% |
The investigate the benefit of a focal lesion ablative microboost in prostate cancer (FLAME) trial (ClinicalTrials.gov identifier NCT01168479) is a phase III study evaluating an EBRT boost to the DIL [49]. The tumor TARGET PC trial is a nonrandomized phase II study (ClinicalTrials.gov identifier, NCT01802242) comparing a combination of a boost to the DIL with high-dose-rate brachytherapy and a moderate dose of volumetric modulated arc therapy (VMAT ) for the rest of the prostate, with VMAT as monotherapy for the whole prostate.
16.4 Hypofractionation/Stereotactic Body Radiotherapy
Larger fraction per treatment is hypothesized with better radiobiological effect in the treatment of PC [50]. In addition to that, the potentially low alpha/beta ratio of PC is hypothesized as the rationale of hypofractionation and SBRT [51–53]. In moderate hypofractionation, 2.2–4 Gy per fraction is generally delivered with linear accelerators, while doses above 5 Gy are used in SBRT. SBRT uses more intensive immobilization and tracking systems to safely deliver high doses of radiation compared to IMRT .
SBRT and hypofractionation studies generally investigated low-risk and intermediate-risk patients. Because high-risk disease requires more comprehensive approach due to risk of regional spread, SBRT is generally used as boost in such patients. Also, greater likelihood of local recurrence and resistance of conventional RT dose makes high-risk patients a candidate for dose escalation with larger RT fraction [54].
Summaries of hypofractionation and SBRT studies are depicted in Table 16.3. Briefly, SBRT and hypofractionated RT could be used as monotherapy, whole-gland boost therapy, or focal boost of IPL. There are various RT schemes for monotherapy of PC, but the optimal fractionation has not been determined. Most of the studies investigated the BPFS, quality of life (QoL), and toxicity. In general, hypofractionation or SBRT is well tolerated with acceptable results without any serious increase in toxicity.
Table 16.3
Published studies of stereotactic radiotherapy and hypofractionation in prostate cancer treatment
Author | Year | n | Design | Risk group | Fractionation | Therapy | Follow-up | Outcome | Toxicity |
|---|---|---|---|---|---|---|---|---|---|
Arcangeli et al. | 2011 | 168 | Randomized | HR | Conv. vs 3.1 Gy × 20 fr | Monotherapy | 70 months | 5y BPFS 79–85% No difference | Late Grd 2 ≥ 11–17% No difference |
Pollack et al. | 2013 | 303 | Randomized | HR
Related posts: Quality Assurance of Modern Radiotherapy Techniques in Prostate Cancer Treatment Quality Assurance of Modern Radiotherapy Techniques in Prostate Cancer Treatment
 Guidelines for the Delineation of Lymphatic Target Volumes in Prostate Cancer Guidelines for the Delineation of Lymphatic Target Volumes in Prostate Cancer
 Prostate Cancer Risk Grouping and Selection Criteria Based on Radiation Oncology Perspective Prostate Cancer Risk Grouping and Selection Criteria Based on Radiation Oncology Perspective
 Proton Therapy for the Treatment of Prostate Cancer Proton Therapy for the Treatment of Prostate Cancer
 Functional Imaging-Guided Radiotherapy and Radiolabelled Targeted Therapies in Prostate Cancer Functional Imaging-Guided Radiotherapy and Radiolabelled Targeted Therapies in Prostate Cancer
 Stereotactic Body Radiotherapy for Prostate Cancer Stereotactic Body Radiotherapy for Prostate Cancer
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|