Adductor Muscle Group (Medial Thigh) Resection
Jacob Bickels
Yair Gortzak
Martin M. Malawer
Yehuda Wolf
BACKGROUND
The adductor compartment of the thigh is the second most common site for soft tissue tumors of the thigh, preceded by the anterior (quadriceps) compartment. Although resection of the muscular elements of this compartment does not considerably affect overall function of the lower extremity, the proximity of the major neurovascular bundle (NVB) of the lower extremity requires special attention in the preoperative evaluation process and during tumor resection.
Tumors arising within the adductor compartment are often extremely large at presentation. As they enlarge, they often displace the superficial femoral and profundus vessels, and they may involve the extrapelvic floor musculature (obturator fascia) and bone (superior and inferior pubic rami and ischium) and even extend extracompartmentally to the medial hamstrings or the psoas muscle and the adjacent hip joint. These anatomic characteristics often make resection extremely difficult. Such large tumors were traditionally treated with amputation (ie, hemipelvectomy). Availability of effective chemo- and radiotherapeutic regimens has allowed the execution of limb-sparing resections at that site with low rates of local tumor recurrence.
Lipomas and low-grade liposarcomas, which are the most common tumor type at that site, are usually removed easily with their enveloping capsule without having to manipulate the vascular bundle. High-grade soft tissue sarcomas, however, may grossly adhere to and surround the vascular bundle and require partial or complete resection of the involved bundle segment. Therefore, a limb-sparing tumor resection at that site begins with dissection and preservation of the superficial femoral vessels.
Large high-grade sarcomas usually necessitate ligation of the profundus femoris artery. The surrounding adductors are then detached from their origin along the inferior and superior pubic rami and ischium and removed en bloc with the tumor. Reconstruction of the soft tissue defect remaining after tumor resection is usually done by transferring the sartorius muscle and the remaining medial hamstrings.
ANATOMY
The adductor compartment of the thigh consists of the adductor magnus, brevis, and longus; the gracilis muscles; and the major vascular bundle of the lower extremity. Compartmental muscles arise from the pelvic floor and the medial aspect of the ipsilateral pelvic ring (symphysis pubis, inferior pubic ramus, ischium, and obturator fascia) and attach distally to the linea aspera and the medial aspect of the distal femur.
The superficial femoral artery passes along the anterior and lateral margins of the entire compartment and forms the lateral border. This compartment is best thought of as an inverted funnel, with the base being the obturator ring and fascia, the lateral border being the femur and linea aspera, and the tip of the cone being the adductor hiatus (FIG 1).
INDICATIONS
Benign soft tissue tumors of the adductor compartment
Soft tissue sarcomas of the adductor compartment
CONTRAINDICATIONS
Approximately 95% of high-grade soft tissue sarcomas and almost all low-grade sarcomas of the adductor group can be safely resected.
Today, amputation is rarely indicated. There are, however, several contraindications to limb-sparing surgery.
In general, a combination of several contraindications is required, most of which are related to extremely large tumors. In those cases, we recommend induction chemotherapy or isolated limb perfusion and repeated staging studies before a definitive decision is made regarding amputation.2,3
Contraindications to limb-sparing surgery include the following:
Major neurovascular involvement
Pelvic floor involvement
Extensive extracompartmental extension
IMAGING AND OTHER STAGING STUDIES
Preoperative staging studies must evaluate the sartorial canal, pelvic floor, medial hamstrings, ischium, psoas muscle, and hip joint to determine the full extent of bone and soft tissue involvement; plain radiographs, computed tomography (CT), and magnetic resonance imaging (MRI) of the affected thigh, ipsilateral hip joint, and hemipelvis are indicated.
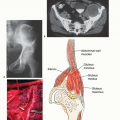
Most adductor tumors displace the superficial femoral vessels but rarely directly involve these structures (FIG 2). The profundus femoris artery, on the other hand, is often involved and must be ligated as it passes through the adductor brevis. The obturator artery and nerve, which pass through the obturator fascia, are routinely ligated.
In light of the earlier discussion, preoperative vascular evaluation of the patient should include direct questioning about intermittent claudication, limb swelling, and deep vein thrombosis. Vascular evaluation should include, in addition to physical examination, ankle-brachial pressure index and duplex ultrasound scanning of the femoral arteries and veins in the affected leg and of the greater saphenous vein in both legs.
Underlying chronic obstructive arterial disease should prompt liberal use of angiography, CT angiography, or magnetic resonance (MR) angiography. Biplanar angiography,
especially in patients older than 40 years of age, should be done to evaluate the patency of the superficial femoral artery: Ligation of the profundus artery without a patent superficial femoral artery will lead to a nonviable extremity.
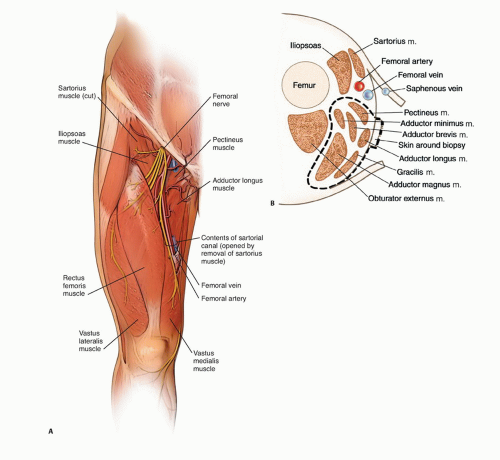
FIG 1 • A. Anatomic structures of the adductor compartment. B. Crosssectional anatomy of the adductor group. The sartorial canal is opened.
In the past, angiography was also used preoperatively to outline the course of the vascular bundle within the affected thigh and to assess the likelihood of vascular reconstruction. Highdefinition MR scans provide the same useful information.Related posts:
 Biopsy of Musculoskeletal Tumors
Biopsy of Musculoskeletal Tumors
 Overview of Resections around the Shoulder Girdle
Overview of Resections around the Shoulder Girdle
 Primary and Metastatic Tumors of the Spine: Total En Bloc Spondylectomy
Primary and Metastatic Tumors of the Spine: Total En Bloc Spondylectomy
 Surgical Management of Metastatic Bone Disease: Pelvic Lesions
Surgical Management of Metastatic Bone Disease: Pelvic Lesions
 Hamstrings Muscle Group (Posterior Thigh) Resection
Hamstrings Muscle Group (Posterior Thigh) Resection
 Distal Femoral Resections with Endoprosthetic Replacement
Distal Femoral Resections with Endoprosthetic Replacement

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


