These men ask for just the same thing, fairness, and fairness only. This, so far as in my power, they, and all others, shall have.
—Abraham LincolnAbraham Lincoln, 16th U.S. president
Introduction
Primary care providers see patients of all ages, ethnicities, sexual orientations, educational levels, psychological profiles, and religious beliefs. This chapter examines how being culturally competent can optimize care management for virtually all patients afflicted with diabetes.
Cultural competency is defined as having “awareness of and sensitivity to cultural differences; knowledge of cultural values, beliefs, and behaviors; and skill in working with culturally diverse populations.”1 The first step in developing cultural competency is understanding the distinction between race and culture. Race refers to specific populations defined by unique physical characteristics, whereas culture refers to the shared beliefs, values, customs and behaviors of specific populations.
Although race and culture are often interrelated, there is a tendency to stereotype patients’ cultural influences based solely upon their race. This can result in misunderstanding and miscommunication because patients of different races may, in fact, share the same culture. For example, Cuban Americans represent several races—Africans, Latinos and whites—yet, they are all influenced by the shared values and customs associated with Cuban culture.
The characteristics that best define a culturally competent provider include (1) one whose practice is based upon value diversity, (2) one who has the capacity and willingness for cultural diversity self-assessment, (3) one who possesses a knowledge base that includes the fundamental philosophical, religious, and family values related to the cultural groups to which treatment is rendered, and (4) one who adapts one’s professional service delivery to reflect the needs of the cultures that are being treated.
Valuing diversity implies that one has accepted and developed a respect toward cultural and ethnic differences. Not all ethnic groups respond equally to evidence-based treatment protocols. Asian Americans, for example, are highly insulin resistant despite having a physical appearance that suggests ideal metabolic functioning.
Traditions that have been passed on through generations may strongly influence a patient’s approval of therapeutic options. Adherence to prescribed therapies is greatly influenced by family dynamics, religious beliefs, immigrant status, and literacy comprehension rates. During the Islamic calendar’s holy month of Ramadan, Muslims fast from dawn to sunset, a gesture that is thought to figuratively burn away all sins. Yet this can be a challenge for Muslims with diabetes: a large epidemiologic study conducted in 13 Islamic countries on 12,243 individuals with diabetes who fasted during Ramadan showed a high rate of acute complications (DKA, hypoglycemia, dehydration and thrombosis).2Table 14-1 presents recommendations for managing glycemic control in Muslim patients during fasts.
Cultural self-assessment implies that a conscious effort be made by the practitioner to customize interviewing and physical examining techniques consistent with the patient’s ethnic, cultural, and religious values. The most important actions that must be adopted during cultural diversity training are usually taken for granted. For instance, comfortable physical distance during social interactions varies by culture. Sitting too far away from a gay couple could infer an anxious attitude on the part of the examiner. Elderly Native American patients will typically discourse in a slow speech pattern that may also make the examiner feel uncomfortable and hurried. Yet attempting to speed up the conversation would be a sign of disrespect.
Even shaking hands with a patient upon entering the room may influence how the clinician is perceived from a cultural perspective. In some cultures, an excessively firm grip on a patient’s hand is perceived as an attempt to demonstrate intellectual and personal superiority over that individual, whereas use of a lighter grip suggests equality.
TABLE 14-1. Suggested Guidelines for Managing Diabetes during Ramadan and Public Fasting Days on the Jewish Calendar
• Frequent blood glucose self-monitoring is required of all patients using insulin.
• The common practice of ingesting large amounts of foods rich in carbohydrate and fat, especially at the sunset meal, should be avoided. Because of the delay in digestion and absorption, ingestion of foods containing “complex” carbohydrates may be advisable at the predawn meal, while foods with more simple carbohydrates may be more appropriate at the sunset meal.
• Normal levels of physical activity may be maintained. However, excessive physical activity may lead to higher risk of hypoglycemia and should be avoided, particularly during the few hours before the sunset meal.
• Patients must immediately end the fast if they become hypoglycemic (blood glucose, 60 mg/dL) or if the blood glucose level reaches <70 mg/dL within the first few hours of initiating the fast especially if insulin or a sulfonylurea is being used.
• No fasts should be undertaken on “sick days.”
• Use of a medical alert bracelet is strongly encouraged.
• Patients with wide glycemic variability should not fast.
• Patients with T1DM who insist on fasting should be placed on an insulin pump and a continuous glucose sensor, which will alarm in response to either a rapid decrease in blood glucose or an actual hypoglycemic event.
• In patients with T2DM who are well controlled with diet alone, the risk associated with fasting is quite low. However, there is still a potential risk for occurrence of postprandial hyperglycemia after the predawn and sunset meals if patients overindulge in eating. Distributing calories over two to three smaller meals during the non-fasting interval may help prevent excessive postprandial hyperglycemia.
• Elderly patients should consume extra fluids during non-fasting times to minimize the risk of dehydration and thrombosis.
Adapted from Al-Arouj M, Bouguerra R, Buse J, et al. Recommendations for management of diabetes during ramadan. Diabetes Care. 2005;28(9):2305-2311.
Cultural self-assessment takes time and practice. Patient clinicians will learn how effective use and interpretation of “body language” may be used to their advantage to improve patients’ diabetes care.
Many factors may influence cross-cultural (clinician vs. patient) interactions. For example, biases based on historical cultural experiences can explain some patients’ reluctance to comply with chronic care interventions. Some Native American tribal members may blame the “white man” for bringing diabetes to their people, while anyone who remembers the “Tuskegee Study of Untreated Syphilis in the Negro Male” can see that ethnicity can affect standards of care. This study, conducted by the Public Health Service in 1932, attempted to record the natural history of syphilis in hopes of justifying a treatment programs for blacks. The study initially involved 600 black men—399 with syphilis and 201 who served as “healthy controls.” The study was conducted without the benefit of patients’ informed consent. Researchers told the men they were being treated for “bad blood,” a local term used to describe several ailments, including syphilis, anemia, and fatigue. However, patients never received treatment for syphilis. This study, which was originally projected to last 6 months, was continued for over 40 years. When penicillin became the drug of choice for treating syphilis in 1947, researchers did not provide this treatment option to the Tuskegee subjects. In 1974, a $10 million out-of-court settlement was reached. As part of the settlement, the U.S. government promised to give lifetime medical benefits and burial services to all living participants.3 The Tuskegee Study led to important federal regulations related to human clinical trials. All patients who participate in a clinical trial are now required to sign informed consent. Institutional Review Boards (IRBs) provide oversight and protection for all subjects who participate as volunteers in human clinical trials.
The integration of ethnic and cultural dynamics into one’s practice will relax patient barriers toward diabetes self-management. Culturally competent practices are able to provide unique services to patients suffering from a globally epidemic disorder. Medical practices that service diverse populations will certainly grow as a result of their attempts to become culturally competent.
Estimates of complementary and alternative medicine (CAM) use in individuals with diabetes are comparable to those with other common chronic medical disorders.4 In one study, 57% of individuals with diabetes who used CAM discussed it with their regular physician and 43% were actually referred to CAM users by a physician.4 This is reassuring because it means that patients with diabetes are not abandoning conventional treatments, which have been rigorously tested, for unconventional treatments, which lack properly designed efficacy trials. Enterprising PCPs will acknowledge CAM use by their patients and allow them to incorporate modalities that may augment traditional therapeutic options.
Culturally competent practices should strive to develop tools that enhance education of divergent patient populations. Group diabetes classes targeting specific ethnic or religious populations within a given community may be developed. (See Chapter 1 for tips on establishing group diabetes visits.). Certified Diabetic Educators may be selected to assist with the group sessions. High-risk patients who attend the group sessions may even be screened for diabetes complications that are highly prevalent within that selected patient population. The possibilities for enhancing one’s practice by targeting cultural competency are electrifying and well within the realm of primary care.
Barriers to Health Care
Many minority populations face cultural obstacles to the acquisition of health care. Although some assume that the American system of health care is universally accepted and accessible, for a variety of reasons, ethnic minorities receive suboptimal care in the United States. Barriers to care include patients’ and providers’ cultural beliefs and misalignment between the American health-care system and culturally based health assumptions.
• Delays in Seeking Health Care
Delays in seeking care in a timely manner are an essential barrier and may be culturally based. Some cultures believe that diabetes indicates a failure to live properly, represents a lack of spiritual strength, or is a punishment for immoral behavior.1 Patients who resist seeking health care because they associate illness with a morally inferior lifestyle deny themselves timely access to care.
• Cultural Beliefs versus American Health-care Attitudes
Violation of cultural ideals by American health-care attitudes is another barrier against early diabetes diagnosis and intensive therapeutic intervention. Sound diabetes management is based upon integrating healthy lifestyle choices with appropriate and timely pharmacologic therapies. In the ideal world, patients should eat well balanced meals, exercise for 30 minutes 5 days a week, lose 7 to
10 lb when advised to do so by their physician and get 6 to 8 hours of uninterrupted sleep each night. Doctors expect that all of their patients should become phenotypic clones of the late Jack LaLanne after one to two consultations. If everyone in the world possessed Jack LaLanne’s genetic good fortune, there would probably be no need for physicians!
Cultural diversity demands that clinicians carefully assess each patient to determine their individual glycemic and metabolic baseline and targeted goals. An Asian American patient, for example, may have a BMI of only 24 kg per m2, yet be diagnosed with diabetes and hypertriglyceridemia. This hesitant patient may even argue his or her case against having diabetes by saying, “I thought only heavy people have diabetes and I’m not even overweight!”
The clinician will need to be forthright in explaining the ethnic differences in BMIs between Asians and non-Asian Americans. Non-white Hispanics may view slight obesity as a sign of being healthy rather than carrying risk for diabetes or cardiovascular disease (CVD).1 Although much evidence links obesity and T2DM, patients who consider weight control measures to be contrary to their cultural ideals may devalue the advice of their physician. PCPs must exercise care in offering health-care advice to their patients to avoid conflicts between their patients’ cultural beliefs and any preexisting notions of the superiority of the traditional American approach to medical care.
Race and Racial Disparities
• Diabetes Prevalence
Diabetes touches Americans from all walks of lives. The defenseless pancreatic β-cell is an equally opportunistic target of apoptosis and disease progression regardless of age, race, gender, family history, or lifestyle choices. That being said, certain ethnic populations are disproportionately affected by diabetes. The prevalence of diabetes is two to six times higher among Hispanic Americans, African Americans, Native Americans, and Asian Americans than among white Americans. The National Institutes of Health reports that Native Americans are 2.2 times more likely to have diabetes than are non-Hispanic whites.5 Even among Native Americans, diabetes prevalence rates vary, ranging from 6% in Alaskan Natives to 29.3% in the Pima Indians living in southern Arizona.5
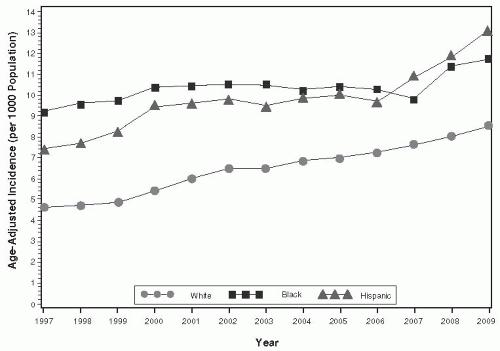
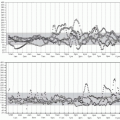
From 1997 to 2009 the age-adjusted incidence of diagnosed diabetes was 8.5/1,000 among whites, 11.7/1,000 among blacks, and 13.1/1,000 among Hispanics in patients aged 18 to 79 as shown in Figure 14-1. The prevalence of diabetes by race from 1980 to 2009 is shown in Figure 14-2.
Trends in immigration suggest that the number of Latino, African, and Asian Americans will rise. Currently, Latino Americans make up 12.5% of the population, followed by African Americans at 12.3%, and Asian Americans at 3.6%. By 2050, 30% of the U.S. adult population will have diabetes. Thus, the number of adults aged 20 and older with diabetes will have increased 165% from 11 million (prevalence of 4%) in 2000 to 29 million in 2050. The fastest growing ethnic group with diagnosed diabetes is expected to be black males (+363% from 2000 to 2050), with black females (+217%), white males (+148%), and white females (+107%) following.6
Figure 14-1 • Age-Adjusted Incidence of Diagnosed Diabetes per 1,000 Population Aged 18 to 79 Years by Race/Ethnicity in the United States 1997 to 2009.
Reference: Centers for Disease Control and Prevention. Data and Trends. http://www.cdc.gov/diabetes/statistics/incidence/fig6.htm. Accessed January 8, 2012.
• Metabolic Parameters
Successful management of diabetes requires implementation of the most appropriate lifestyle and pharmacologic interventions that will allow each patient to achieve his or her customized glycemic, blood pressure, and cholesterol targets. Epidemiologic data suggest that metabolic parameters are achieved more often among white patients with diabetes than blacks and non white Hispanics.7
Working with patient data from a large managed care population, Brown and colleagues found that mean A1C was significantly higher among Latinos (8.1%, p < 0.0001), Asians/Pacific Islanders (8.1%, p < 0.0001), and African Americans (7.9%, P = 0.0009) than among white Americans (7.7%). Mean LDL was higher among African Americans than among white Americans (118 vs. 111 mg per dL, p < 0.0001), and African Americans were also more likely to have inadequate blood pressure control (greater than 140/90 mm Hg) than were white Americans (55.5% vs. 44.1%, p < 0.0001).
• Physiologic Disparities
Although practice guidelines for the diagnosis and management of diabetes provide a valuable resource for physicians, they often fail to emphasize key physiologic differences among the various ethnic populations that can impact care. For example, first-generation Asian Americans tend to have lower body weight and BMI measurements, yet they have a greater prevalence of T2DM than the general population. Compared with whites, Asian Americans are more likely to be overweight but less likely to be obese after applying the modified Asian criteria (Table 14-2). Yet, considered as an ethnic population, Asian Americans are approximately 30% more likely to have T2DM than their white counterparts.8 PCPs who fail to screen for diabetes in Asian American patients having a BMI of ≥23 kg per m2 could miss the diagnosis in this high-risk population.
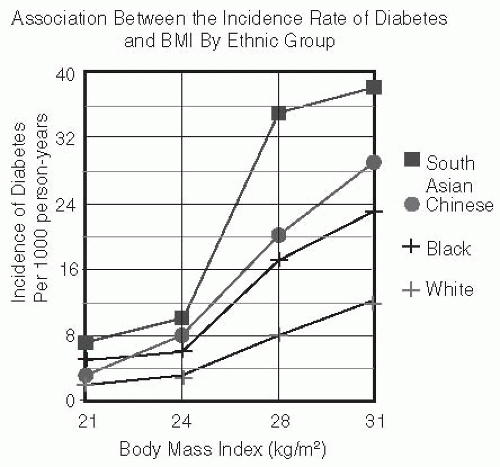
Even at BMI ranges thought to be acceptable, the risk of diabetes may be markedly underestimated in non-white ethnic groups, several of which appear to be particularly sensitive to weight gain in terms of diabetes risk. As shown in Figure 14-3, for the equivalent incidence of diabetes at BMI of 30 kg per m2 for white subjects, the BMI cutoff values are 24 for South Asians, 25 for Chinese, and 26 for black subjects.9 A population shift from the normal to the obese BMI range could theoretically result in a 12-fold increase in the incidence of diabetes among the Asian population groups compared with a four- to sixfold increase in diabetes in other ethnic groups.
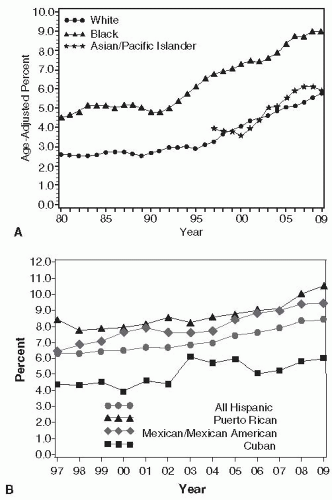
Figure 14-2 • A. Prevalence of Diabetes Among Whites, Blacks, and Asian/Pacific Islanders from 1980 to 2009. B. Prevalence of Diabetes Among Non white Hispanic Populations from 1997 to 2009.
Reference: Centers for Disease Control and Prevention. Data and Trends. http://apps.nccd.cdc.gov/DDTSTRS/default.aspx. Accessed January 9, 2012.)
TABLE 14-2. National Heart, Lung, and Blood Institute and World Health Organization Guidelines for Defining Obesity
BMI (kg/m2)
Obesity Category
Asian Standard (kg/m2)
<18.5
Underweight
<18.5
18.5-24.9
Normal weight
18.5-22.9
25 to <30
Overweight
23 to <27.5
>30
Obese
>27.5
From World Health Organization Expert Consultation. Appropriate body-mass index for Asian populations and its implications for policy and intervention strategies. Lancet. 2004;363:157-163.
NHLBI Obesity Education Initiative: http://www.nhlbi.nih.gov/guidelines/obesity/prctgd_c.pdf. Assessed January 9, 2012.
Figure 14-3 • For the equivalent incidence rate of diabetes at BMI of 30 kg per m2 for white subjects, the BMI cutoff values are 24 for South Asians, 25 for Chinese, and 26 for black subjects. (Adapted from Chiu M, Austin PC, Manuel DG, et al. Deriving ethnic-specific BMI cutoff points for assessing diabetes risk. Diabetes Care. 2011;34:1741-1748.)
Several hypotheses have been suggested to explain why Asian Americans may have a higher risk of diabetes than other ethnic groups. Asians may be more susceptible to inheritance of the “thrifty gene” because their ancestors were more likely to be exposed to extended periods of starvation. The thrifty gene was advantageous during feast or famine cycles as it enabled individuals to store calories more efficiently as food became scarce. Today, where high-fat and high-calorie foods are readily accessible, the thrifty gene may make weight control difficult under non-starvation conditions.10
Genetic susceptibility to insulin resistance as well as higher central adiposity at similar BMI levels also favors increased risk of developing T2DM in Asians. Adaptation of the sedentary Western lifestyle has undoubtedly promoted a trend toward diabetes on a global scale. Each 2-hour per day increment of time spent watching television is associated with a 14% increase in diabetes risk, whereas each 1-hour per day of brisk walking reduces the risk of diabetes by 34%.11 In all ethnic populations, the diabetes epidemic may be contained simply by having at-risk patients incorporate weight management and moderately intense exercise into their daily routines. Primary prevention of T2DM should become a global primary care initiative.
Quality Improvement in Medical Care Delivery May Not Lead to More Equitable Care for Patients With Diabetes
In the ideal world, physicians attempt to improve the quality, expand access, and eliminate disparities in their health-care delivery. Yet, the improvements observed in health-care quality over the past decade have not translated into more equitable care, because high-risk diabetes population groups are less likely to have access to specialized diabetes care providers.12 NHANES data from 1999 to 2006 suggest that rates of blood pressure control were significantly lower and mean systolic blood pressure was significantly higher for black and non-white Hispanic adults than for white adults with hypertension. Among adults with diabetes, rates of glycemic control were lower and A1C levels were higher for black and non-white Hispanics. Glycemic control was worse for less educated adults. Interestingly, near-universal Medicare coverage for patients after age 65 improved disease control for greater numbers of minorities and less educated adults. This suggests that the underinsured or intermittently insured patients may benefit from acquiring access to some form of health-care coverage.12,13
Patient-centered Diabetes Care-based Cultural and Religious Diversity
The foundation of effective chronic disease management relies upon effective communication between patients and their providers. Cultural competency becomes the ally of the clinician, who may increase the health literacy of his or her diverse patient population. Culturally competent clinicians develop flexibility toward their personal attitudes and beliefs, which helps direct their patients toward achieving their targeted metabolic goals. Providers should address both the strengths and weaknesses of each patient’s self-management skill set. Interventions that incorporate ethnic and cultural ideologies are likely to result in successful outcomes.
• Native Americans
Historically, diabetes prevalence rates were very low among Native Americans prior to 1940. The epidemic of T2DM within the Native American population, which began in the 1960s, corresponds with the westernization of many of these tribal members. Daily caloric consumption increased and energy expenditure declined.
In the 1950s, the Cornell University Medical Team provided care and conducted physical examinations for the majority of the members of the Many Farms Navajo community in North Eastern Arizona and found few cases of T2DM. When comparison data were collected once again in 1988, the 168,000 inhabitants at this site were found to be 10 times more likely to have developed diabetes than were members of their previous generation. Key changes in the community included a reliance on the federally subsidized commodities food program that distributed excess farm produce, consisting primarily of refined flour, cheese, lard, and refined sugar. The recent conceptualization of fry bread as a traditional Native American food is largely a result of the commodities food distribution program established by the Agricultural Act of 1949.14 These factors, coupled with a dramatic reduction in physical activity resulting from altered traditional work patterns and greater access to fast foods, have resulted in an epidemic of diabetes in this and other Native American communities.15 Thus, the purchase and donation of surplus commodities by the U.S. government to the Agricultural Department are believed to have triggered the explosive epidemic of diabetes within the Native American population. Prior to 1950, Native Americans were busy farming their own lands and caring for their own needs. Because the Federal Government continues to provide high-fat food to tribes at no cost, the recipients of the free commodities have determined that farming their own lands is no longer cost-effective. Thus, the Federal Government has eliminated all incentives for primary prevention of T2DM by giving this high-risk population free food that is high in fat and carbohydrates! Native Americans stop farming because they cannot compete with the Federal Government. There is little incentive to work within some tribal communities because they are receiving financial support and free medical care from the government. Meanwhile, the aggregate weight of the population increases and boredom begins to set in. People with extra time on their hands may indulge in alcohol intake, which increases their blood pressure and weight even further. Is the white man to blame for increasing the prevalence of diabetes within the Native American population? One could clearly identify why Native Americans might mistrust the “white man.”
The impact of diabetes within the Native American populace is staggering. Native Americans are nearly three times more likely to be diagnosed with diabetes than non-Hispanic whites of similar ages. Up to 70% of Native Americans ages 45 to 74 have diabetes. The incidence of T2DM in Native American youths ages 15 to 19 has increased 54% since 1996.16
Native Americans have a higher prevalence of many of the complications associated with diabetes. The high prevalence of T2DM, combined with a poorer prognosis, contributes to a disproportionately high and increasing diabetes mortality rate among Native American populations. In New Mexico, diabetes-related mortality increased by 564% and 1,110% for Native American men and women, respectively, from 1958 to 1994.17,18 Using the 2005 MarketScan health expenditure for an adult with average risk ($3,050), a U.S. adult with diabetes was estimated to cost approximately $12,800 during 2005 and an American Indian adult with diabetes approximately $19,260.19 Diabetes management alone comprises over 40% of the total federal Indian Health Service (IHS) budget of $1.46 billion.16 The morbidity burden among Native Americans with diabetes far exceeds that of commercially insured U.S. adults with diabetes. Considering the disproportionate burden of T2DM within this ethnic group, primary care interventions should mandate screening high-risk individuals for prediabetes. Those patients identified as having impaired fasting glucose or impaired glucose tolerance should be introduced to a comprehensive program designed to restore normal β-cell function through weight loss, increased physical activity, and intensive pharmacotherapy if one’s A1C exceeds 6.0%. Patients should be advised to discontinue their use of alcohol and nicotine. Obese patients should also be screened for the presence of obstructive sleep apnea (see Chapter 8).
TABLE 14-3. Considerations for Patients of Different Cultural Backgrounds
Ethnic Population
Cultural Modifications Targeting Patient Interviews
Cultural Modifications Targeting Physical Examinations
Belief Systems Related to Diabetes
Cultural Issues that May Conflict with Allopathic Patient Management
Native Americans
Use indirect communication. Rather than respond by saying, “You should” one should say, “Someone with a similar problem as yours would consider this type of treatment…”
Listening is valued over talking.
Slow down when speaking. Long periods of silence between speakers is common. Do not interrupt, especially if the speaker is elderly.
Eye contact is not direct or only briefly direct. Gaze may be directed over the shoulder.
Modesty and privacy are valued. Permission should be obtained before examination of each area. Care should be taken to keep the body covered. In some reservations clothes are removed only if absolutely necessary.
Belief that diabetes results from consuming too much sugar or too much food in general.
Having diabetes indicates a failure to live properly due to a lack of spiritual strength. Patients feel shamed by the diagnosis and are reluctant to tell friends or family
Suggest, “Eat less sugar. Become more active.”
Monitor for use of herbs, some of which can cause hypoglycemia such as nopal (prickly pear cactus) and hintonia (copalquin). Hintonia can also cause liver failure.
Sharing of medicine between family members is common.
Patients may discontinue medications when they “feel better”
“Cost of medications may be a factor in urban or rural areas, where IHS benefits are not available
Patients are taught traditionally to withstand pain for survival. They are generally undertreated for acute and chronic pain.
Some IHS facilities are short on staff, lack efficiency, and do not practice patient-centered care. The time spent waiting to see a midlevel practitioner adds to the frustration that patients feel regarding diabetes self-management.
Asian Americans
Direct interrogation of physicians by patients is a sign of disrespect
Disagreeing with a PCP is disrespectfu
Speak in short, simple sentences
Ask close-ended questions (“yes” and “no”).
“Low touch society.”
Explain what will transpire during a physical exam.
Family obligations trump personal health needs.
Explain that “body is out of balance,” which is affecting the patient’s ability to function normally
Advise family to use foods that “can restore balance.”
Religious teachings suggest that patient developed diabetes due to living a “prior” life of sin. If patient believes in reincarnation, the thought of having diabetes may therefore be embarrassing. The patient will opt against using insulin or checking blood glucose levels in public. Avoid speaking to patients in public about their diabetes.
Monitor for traditional herbal remedies.
Non adherence common due to use of TCM herbs.
African Americans
Eye contact important during the history and any discussion point.
When entering the exam room, do not stand while interviewing patient. Maintain eye level interview to minimize appearance of cultural superiority and affect trust.
Proactively question about erectile dysfunction in men or sexual dysfunction in women.
Prostate exam in males age 40 and up
Higher risk of chronic kidney disease and cancers. Screen when appropriate.
Screen for glaucoma, especially in patients with a positive family history
Some research has shown that African Americans have a strong sense of living in the present, willingly accept obesity as the norm, and express the view that T2DM is hereditary and therefore cannot be prevented.
Elderly patients may be less trusting of physicians. Patients remember the Tuskegee experiment. Trust must be earned.
Belief that religion may have an impact on disease could delay intensification of treatment.
If patient becomes non adherent in regards to medical regimen or home blood glucose monitoring ask patient about financial burden of medications. Consider co-pay cards when appropriate.
Latino American
Indirect eye contact preferred and is a show of “respect” toward the clinician
Start interview with “small talk” rather than rapidly interrogating the patient
Use “proper names” such as Senor or Senora rather than the patient’s first name.
Sit or stand in close proximity to the patient to show respect
Explain link between “stress” and disease.
Explain that improved blood glucose control will likely improve symptomatology (blurred vision, fatigue, erectile dysfunction, parenthesis, nocturia, and reduce dry skin).
Do NOT attempt to scare patients into using medications by mentioning that failure to treat diabetes aggressively is likely to result in long-term complications
When shaking hands with patients, avoid a firm grip as this would imply that the clinician is attempting to “overpower” them. Simply put your hand forward and have the patient apply the pressure.
Anger or strong emotions may predispose one’s body to develop diabetes but is not the specific trigger for inducing acute or chronic hyperglycemia
Herbal remedies often used, but not often disclosed to clinician for fear of being “scolded.”
Patients may adopt a fatalist attitude toward diabetes, believing their future is “in God’s hands.” This may increase likelihood of non adherence.
Observant Jews
Direct communication acceptable and respected
Avoid scheduling appointments on Friday afternoon, which may interfere with the celebration of the Sabbath. Observant Jews may only walk on the Sabbath and may not accept any other mode of transportation.
Modesty and privacy must be respected especially when examining members of the opposite sex. Asking permission when examining patients is suggested. Chaperone, or patient’s husband should be present when examining a female patient.
Patients respect and accept the treatment protocols prescribed by physicians.
Patients believe that their bodies are shrines on loan from God. They must do whatever possible to protect their bodies and keep themselves as healthy as possible.
For patients with no contraindications to prolonged fasting, alterations in insulin and oral agent regimens may be necessary for Jewish holidays, such as Yom Kippur. Using an ultra long basal insulin, such as degludec or IDegAsp might be useful. Insulin pumping may be continued while fasting using the patient’s standard basal rate profile.
LGBT patients
Avoid sitting farther from the patient than necessary
Develop a comfort level using terms such as “husband” “spouse” “wife” “partner”
High risk of alcohol abuse (binge drinking), cigarette smoking, polycystic ovary syndrome, depression, suicide ideation, obesity, HIV, and insulin resistance
Don’t forget pap smears and cancer screening.
Management of diabetes may take a back seat other psychosocial issues.
Patients who are being treated for HIV often have significant insulin resistance.
Binge drinking, common in Lesbian patients with T1DM, can develop severe hypoglycemia.
References
1. Ahn AC, Ngo-Metzger Q, Legedza AT, et al. Complementary and alternative medical therapy use among Chinese and Vietnamese Americans: prevalence, associated factors, and effects of patient-clinician communication. Am J Public Health. 2006;96(4):647-653.
3. American Jewish Diabetes noes Association. http://www.jewishdiabetes.org/alon/kippur_english.pdf. Accessed February 8, 2011.
4. Gavin JR, Wright EE. Building cultural competency for improved diabetes care: African Americans and diabetes. J Fam Pract. 2007;56(9):S22-S28.
5. Caballero EA, Tenzer P. Building cultural competency for improved diabetes care: Latino Americans and diabetes. J Fam Pract. 2007;56(9):S29-S38.
6. Garnero TL. Providing culturally sensitive diabetes care and education for the Lesbian, Gay, Bisexual, and Transgender (LGBT) community. Diabetes Spectrum. 2010;23(3):178-182.
The IHS provides health services to more than 300,000 American Indians and Alaska Natives throughout the United States with diabetes.20 The 2010 IHS annual budget of more than $4.05 billion equates to approximately $2,700 per individual (compared with $6900 per capita personal health-care expenditures for the total U.S. population.21 In 1997, Congress passed legislation to create Special Diabetes Program for Indians (SDPI) to provide additional IHS funding for diabetes prevention and treatment programs, funding nearly 400 diabetes programs in American Indian and Alaska Native communities in 2007.20 Since the enactment of SDPI, intermediate clinical outcomes (e.g., blood glucose, blood pressure, and cholesterol levels) among American Indians and Alaska Natives with diabetes have improved, and the rate of diabetes-related end-stage renal disease has decreased.19
Many Native American tribes (e.g., Ojibwa, Cree, Dakota, Navajo, Kiowa, Ute), believe that diabetes is, in fact, a new disease introduced by the “white man.” Tribal belief is that diabetes results from a state of imbalance caused by consuming too much sugar, overeating, drinking alcohol, and behaving immorally. Because one should strive to follow a righteous and spiritual life, being diagnosed with diabetes may imply a personal failure to achieve a productive and virtuous life. Those afflicted with diabetes may feel ashamed by a diagnosis that they may be reluctant to share openly with family or friends.22
The severity of a chronic illness is judged by the amount of pain, disability, and discomfort it causes. Those who suffer most tend to seek comfort from a spiritual leader’s ritual healing interventions and the use of herbal remedies. Once ritual healings restore balance to one’s mind, body, and spirit a patient will theoretically commit to living a life of humility and harmony. Patients should begin to incorporate healthier lifestyle choices into their daily living with respect to food, physical activity, prayer, sleep, and social relationships.
Herbs widely used in the Southwest and Mexico include those with known hypoglycemic activity, such as nopal (prickly pear cactus), hintonia (copalquin), garlic, and onion (Table 14-4). Unfortunately, some of these agents also have toxic effects. Hintonia, for example, contains pyrrolizidine alkaloids that can cause severe liver damage (Table 14-5).1
Foods are an essential to many religious and social ceremonies. Among most Native American groups, participating in ceremonial feasts is a key component of maintaining tribal identity. For example, the Navajo categorize food as being either “strong” or “fillers.” Strong foods (corn products, mutton, stew, fry bread, beef, coffee) provide satiety, strength for heavy work, and protection against illness. Strong foods are served at social and religious functions and donated to kin in times of need. Fillers include commodities such as cheese, refined flour, and canned meat. Studies have described many reasons for non adherence to dietary recommendations among Native Americans. Members of the Cherokee tribe reported difficulty in using the carbohydrate exchange system as well as a reluctance to incorporate healthier foods and cooking practices in their daily lives.23 For the Navajo and Ute tribes, the suggestion to withhold certain foods, limit their consumption, or not participate in religious feasts is unconscionable. Thus, simply suggesting that Native Americans adopt a totally Western style diet, limit carbohydrates and saturated fats, or increase fiber intake becomes a cultural nightmare, one that is likely to result in distrust toward the prescriber and non adherence by the patient. CDEs specially trained to assist with dietary modification for this special population should be consulted within the IHS system whenever possible.
Introducing cultural competency to clinicians managing Native Americans through the IHS or privately contracted organizations has encountered bureaucratic roadblocks. Some agencies lack professional presence or may be staffed by transient newly trained residents paying back student loans. IHS services are not located in large urban centers. Therefore, Native Americans who seek medical care outside of their local clinics and hospitals are likely to encounter clinicians who have limited or no experience with their culture. Due to budget constraints within the IHS, rationing of care within the system results in gaps and delays in treatment. The end result within IHS creates a program in which diagnoses and treatment interventions are delayed, exacerbating the severity of a patient’s underlying disease state. The inefficiency of the IHS implies that Native Americans may live with more disabling chronic diseases, which will become more costly to manage over time. The U.S. Government Accountability Office (GAO) visited 13 IHS-funded facilities in 2005 and discovered that wait times at 4 IHS-funded facilities ranged from 2 to 6 months for women’s health care, and general physicals. Some patients had to travel over 90 miles one way to obtain care. After waiting all day to see a midlevel practitioner, many patients delay travel until their condition is truly emergent.
Only gold members can continue reading. Log In or Register to continue