Chapter 25
Acquired Immunodeficiency Syndrome
At the conclusion of this chapter, the reader should be able to:
• Describe the etiology and viral characteristics of human immunodeficiency virus (HIV-1).
• Explain the epidemiology, including modes of transmission, and prevention of HIV-1.
• Discuss the signs and symptoms of various stages and the classification of HIV infection.
• Describe the immunologic manifestations and cellular abnormalities of HIV-1 infection.
• Explain the serologic markers and diagnostic evaluation of HIV.
• Compare the features of fourth generations HIV testing to other generations of testing.
• Analyze a representative HIV-1 case study.
• Correctly answer case study related multiple choice questions.
• Be prepared to participate in a discussion of critical thinking questions.
• Describe the principles of the Rapid HIV antibody test, GS HIV Combo Antigen/Antibody EIA, and simulation of HIV-1 Detection.
Etiology
Viral Characteristics
Viral Structure
The HIV-1 virus (Fig. 25-1) is composed of a lipid membrane, structural proteins, and glycoproteins that protrude. The viral genome consists of three important structural components—pol, gag, and env. These gene components code for various products (Table 25-1). Long terminal redundancies (LTRs) border these three components. HIV-2 has a different envelope and slightly different core proteins.
Table 25-1
| Component | Product |
| pol | Produces DNA polymerase |
| Produces endonuclease | |
| gag | Codes for p24 and for proteins such as p17, p9, and p7 |
| env | Codes for two glycoproteins, gp41 and gp120 |
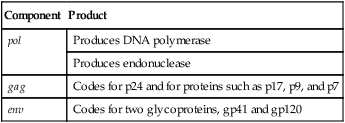
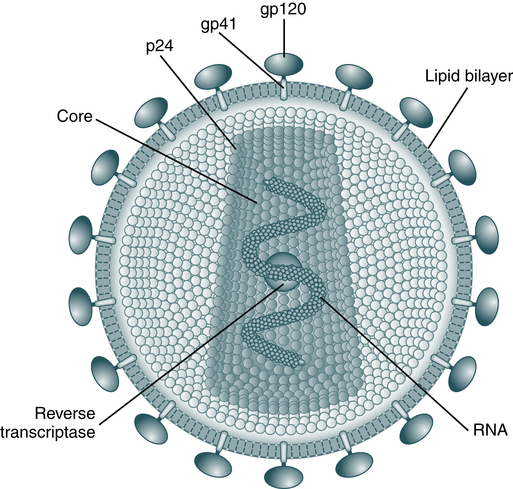
The envelope is made up of glycoproteins (gp) of 120 kDa and 41 kDa. The main core protein is p24. As an RNA virus, it relies on reverse transcriptase to produce complementary DNA for transcription and translation. (From Peakman M, Vergani D: Basic and clinical immunology, ed 2, London, 2009, Churchill Livingstone.)
Cells infected with HIV can be examined with an electron microscope. The virus may appear as buds of the cell membrane particles. The virion has a double-membrane envelope and an electron-dense laminar crescent or semicircular cores. An intermediate, less electron-dense layer lies between the envelope and core. In a mature, free extracellular virion, the core appears as a bar-shaped nucleoid structure in cross section. This structure appears circular and is frequently located eccentrically. It is composed of structural proteins and glycoproteins that occupy the core and envelope regions of the particle. The virion consists of knoblike structures composed of a protein called glycoprotein (gp) 120, which is anchored to another protein called gp41. Each knob includes three sets of these protein molecules. The core of the virus includes a major structural protein called p25 or p24 encoded for by the gag gene. After human exposure, these and other viral components may induce an antibody response important in serodiagnosis (Table 25-2).
Table 25-2
HIV Proteins of Serodiagnostic Importance
| Virus | Protein | Location | Gene |
| HIV-1 | gp41 | Envelope (transmembrane protein) | env |
| gp160/120 | Envelope (external protein) | env | |
| p24 | Core (major structural protein) | gag | |
| HIV-2 | gp34 | Envelope (transmembrane protein) | env |
| gp140 | Envelope (external protein) | env | |
| p26 | Core (major structural protein) | gag |
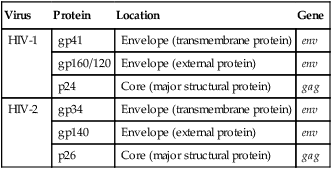
The env gene encodes for a polyprotein that contains numerous glycosylation sites. The glycoprotein gp160 is found on infected cells but is deficient on viral particles; however, gp160 gives rise to two glycoproteins, gp120 and gp41, which are associated with the viral envelope. The encoding genes and gene products, or antigens, of the AIDS virus may induce an antibody response after human exposure (Table 25-3).
Table 25-3
Encoding Genes and Antigens of AIDS Virus
| Encoding Gene | Antigen |
| gag | p55 |
| gag | p24 |
| gag | p17 |
| pol | p66 |
| pol | p51 |
| sor | p24 |
| env | gp160 |
| env | gp120 |
| env | gp41 |
| 3′ orf | p27 |
Viral Replication
The replication of HIV is complicated and involves several steps (Fig. 25-2). The HIV life cycle is that of a retrovirus (Box 25-1). Retroviruses are so named because they reverse the normal flow of genetic information. In body cells, the genetic material is DNA. When genes are expressed, DNA is first transcribed into messenger RNA (mRNA), which then serves as the template for the production of proteins. The genes of a retrovirus are encoded in RNA; before they can be expressed, the RNA must be converted into DNA. Only then are the viral genes transcribed and translated into proteins in the usual sequence.
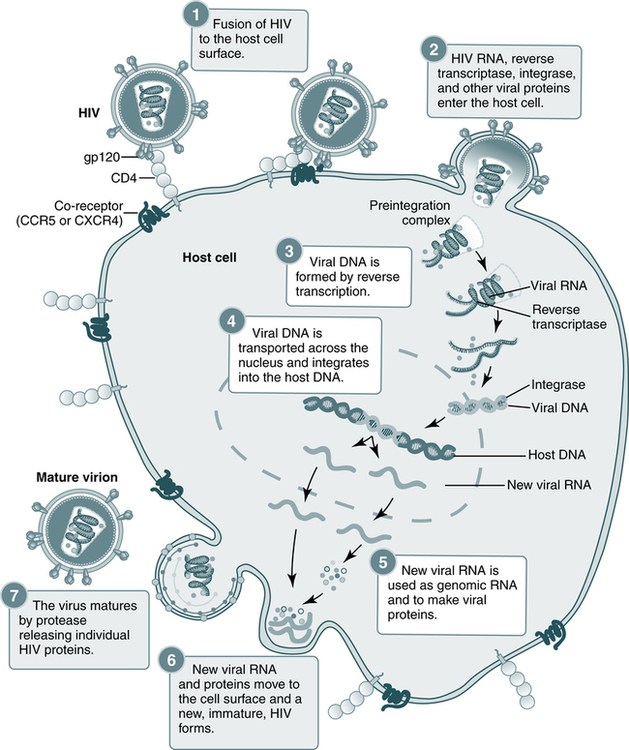
Steps in the HIV replication cycle
1. Fusion of the HIV cell to the host cell surface; 2. HIV RNA, reverse transcriptase, integrase, and other viral proteins enter the host cell; 3. viral DNA is formed by reverse transcription; 4. viral DNA is transported across the nucleus and integrates into the host DNA; 5. new viral RNA is used as genomic RNA and to make viral proteins; 6. new viral RNA and proteins move to the cell surface and a new, immature, HIV virus forms; 7. the virus matures by protease releasing individual HIV proteins. (Courtesy National Institute of Allergy and Infectious Diseases, National Institutes of Health, Bethesda, Md.)
Target Cells
The infectious process begins when the gp120 protein on the viral envelope binds to the protein receptor, called CD4, located on the surface of a target cell. HIV-1 has a marked preference for the CD4+ subset of T lymphocytes (Fig. 25-3). In addition to T lymphocytes, macrophages, peripheral blood monocytes, and cells in the lymph nodes, skin, and other organs also express measurable amounts of CD4 and can be infected by HIV-1. About 5% of the B lymphocytes may express CD4 and may be susceptible to HIV-1 infection. Macrophages may play an important role in spreading HIV infection in the body, both to other cells and to the target organs of HIV. Monocyte-macrophages enable HIV-1 to enter the immune-protected domain of the central nervous system (CNS), including the brain and spinal cord.
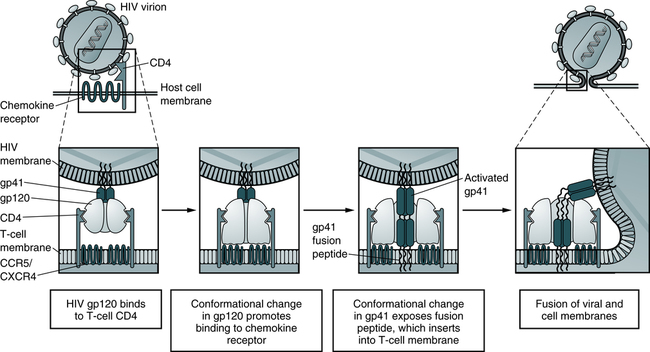
In the model, depicted sequential conformational changes in gp120 and gp41 promote fusion of the HIV-1 and host cell membranes. The fusion peptide of activated gp41 contains hydrophobic amino acid residues that promote insertion into the host cell plasma membrane lipid bilayer. (Adapted from Abbas AK, Lichtman AH, Pillai S: Cellular and molecular immunology, ed 6, Philadelphia, 2007, Saunders.)
Replication
Retroviruses carry a single, positive-stranded RNA and use reverse transcriptase to convert viral RNA into DNA. The life cycle of the HIV-1 virus consists of five phases (see Box 25-1):
1. The virus attaches and penetrates target cells (e.g., lymphocytes) that express the CD4 receptor. After penetration, the virus loses its protein coat, exposing the RNA core.
2. Reverse transcriptase converts viral RNA into proviral DNA.
3. The proviral DNA is integrated into the genome (genetic complement of the host cell).
4. New virus particles are produced as a result of normal cellular activities of transcription and translation.
Epidemiology
Classification System
The revised definition of HIV infection, which applies to both HIV-1 and HIV-2, incorporates the reporting criteria for HIV infection and AIDS into a single case definition (Box 25-2). The revised HIV criteria apply to AIDS-defining conditions for adults and children that require laboratory evidence of HIV.
Laboratory Criteria for HIV Infection
• Positive result from an HIV antibody screening test (e.g., reactive enzyme immunoassay [EIA∗]) confirmed by a positive result from a supplemental HIV antibody test (e.g., Western blot or indirect immunofluorescence assay test).
• Positive result or report of a detectable quantity (i.e., within the established limits of the laboratory test) from any of the following HIV virologic (i.e., non-antibody) tests†:– HIV nucleic acid (DNA or RNA) detection test (e.g., polymerase chain reaction [PCR])– HIV p24 antigen test, including neutralization assay– HIV isolation (viral culture)
• CD4+ T-lymphocyte count of <200 cells/µL or CD4+ T-lymphocyte percentage of total lymphocytes of <14 or documentation of an AIDS-defining condition (see Appendix A). Documentation of an AIDS-defining condition supersedes a CD4+ T-lymphocyte count of >200 cells/µL and a CD4+ T-lymphocyte percentage of total lymphocytes of >14. Definitive diagnostic methods for these conditions are available in Appendix C of the 1993 revised HIV classification system and the expanded AIDS case definition (2) and from the National Notifiable Diseases Surveillance System (available at http://www.cdc.gov/epo/dphsi/casedef/case_definitions.htm).
2008 Surveillance Case Definition for HIV Infection Among Children Aged <18 Months
 – HIV p24 antigen test, including neutralization assay, for a child aged >1 month– HIV isolation (viral culture)
– HIV p24 antigen test, including neutralization assay, for a child aged >1 month– HIV isolation (viral culture)Laboratory Criterion for Presumptive HIV Infection
• Positive results on one specimen (not including cord blood) from the listed HIV virologic tests (HIV nucleic acid detection test; HIV p24 antigen test, including neutralization assay, for a child aged >1 month; or HIV isolation [viral culture] for definitively HIV infected) and no subsequent negative results from HIV virologic or HIV antibody tests.
• HIV infection diagnosed by a physician or qualified medical-care provider based on the laboratory criteria and documented in a medical record. Oral reports of prior laboratory test results are not acceptable.
• When test results regarding HIV infection status are not available, documentation of a condition that meets the criteria in the 1987 pediatric surveillance case definition for AIDS.
Laboratory Criteria for Uninfected With HIV, Definitive
• At least two negative HIV DNA or RNA virologic tests from separate specimens, both of which were obtained at age ≥1 month and one of which was obtained at age ≥4 months.
• At least two negative HIV antibody tests from separate specimens obtained at age >6 months.
• No other laboratory or clinical evidence of HIV infection (i.e., no positive results from virologic tests [if tests were performed] and no current or previous AIDS-defining condition)
Laboratory Criteria for Uninfected With HIV, Presumptive
• Two negative RNA or DNA virologic tests, from separate specimens, both of which were obtained at age ≥2 weeks and one of which was obtained at age ≥4 weeks.#
• One negative RNA or a DNA virologic test from a specimen obtained at age ≥8 weeks.
• One negative HIV antibody test from a specimen obtained at age ≥6 months.
• One positive HIV virologic test followed by at least two negative tests from separate specimens, one of which is a virologic test from a specimen obtained at age ≥8 weeks or an HIV antibody test from a specimen obtained at age ≥6 months.
• No other laboratory or clinical evidence of HIV infection (i.e., no subsequent positive results from virologic tests if tests were performed, and no AIDS-defining condition for which no other underlying condition indicative of immunosuppression exists).
• Determination of uninfected with HIV by a physician or qualified medical-care provider based on the laboratory criteria and who has noted the HIV diagnostic test results in the medical record. Oral reports of prior laboratory test results are not acceptable.
• No other laboratory or clinical evidence of HIV infection (i.e., no positive results from virologic tests [if tests were performed] and no AIDS-defining condition for which no other underlying condition indicative of immunosuppression exists).
• Positive result from a screening test for HIV antibody (e.g., reactive EIA), confirmed by a positive result from a supplemental test for HIV antibody (e.g., Western blot or indirect immunofluorescence assay).
• Positive result or a detectable quantity by any of the following HIV virologic (non-antibody) tests††:– HIV nucleic acid (DNA or RNA) detection (e.g., PCR)– HIV p24 antigen test, including neutralization assay– HIV isolation (viral culture)
 HIV nucleic acid (DNA or RNA) detection tests are the virologic methods of choice for the diagnosis of exclusion of infection in children aged <18 months. Although HIV culture can be used, culture is less standardized and less sensitive than nucleic acid detection tests. The use of p24 antigen testing to exclude infection in children aged <18 months is not recommended because of poor sensitivity, especially in the presence of HIV antibody. Commercial tests for RNA and DNA detection have become widely available. Quantitative RNA tests have been approved by the Food and Drug Administration (FDA) for monitoring HIV infection, and qualitative RNA tests have been approved to aid diagnosis. The quantitative and qualitative RNA tests meet FDA standards for high analytic and clinical sensitivity and specificity (14-16). All available tests detect the subtypes of group M and strains of group O. HIV-2 can be diagnosed with HIV-2 DNA PCR. HIV RNA tests sometimes do not detect HIV-2 because the viral loads in some HIV-2–infected persons are below detectable levels. Because of the possibility of mutation or recombination involving the sequences detected by a particular test, occasionally, virus might not be detected in a specimen from an HIV-2 infected individual. If HIV-2 infection seems likely but results are negative, testing with a different assay might be advisable.
HIV nucleic acid (DNA or RNA) detection tests are the virologic methods of choice for the diagnosis of exclusion of infection in children aged <18 months. Although HIV culture can be used, culture is less standardized and less sensitive than nucleic acid detection tests. The use of p24 antigen testing to exclude infection in children aged <18 months is not recommended because of poor sensitivity, especially in the presence of HIV antibody. Commercial tests for RNA and DNA detection have become widely available. Quantitative RNA tests have been approved by the Food and Drug Administration (FDA) for monitoring HIV infection, and qualitative RNA tests have been approved to aid diagnosis. The quantitative and qualitative RNA tests meet FDA standards for high analytic and clinical sensitivity and specificity (14-16). All available tests detect the subtypes of group M and strains of group O. HIV-2 can be diagnosed with HIV-2 DNA PCR. HIV RNA tests sometimes do not detect HIV-2 because the viral loads in some HIV-2–infected persons are below detectable levels. Because of the possibility of mutation or recombination involving the sequences detected by a particular test, occasionally, virus might not be detected in a specimen from an HIV-2 infected individual. If HIV-2 infection seems likely but results are negative, testing with a different assay might be advisable.Adapted from Centers for Disease Control and Prevention: Revised Surveillance Case Definitions for HIV Infection Among Adults, Adolescents, and Children Aged <18 Months and for HIV Infection and AIDS Among Children Aged 18 Months to <13 Years—United States, 2008. MMWR 57(RR10);1-8, December 5, 2008.
Infectious Patterns
HIV-1
The progression of the natural history and immunopathogenesis of HIV-1 infection can be demonstrated in six discrete stages (Fig. 25-4). These stages are based on the sequential appearance in plasma of HIV-1 viral RNA, the gag p24 protein antigen, antibodies that bind to fixed viral proteins. No matter how HIV-1 was acquired, the timing of the appearance of viral and other markers of infection is generally uniform and follows an orderly pattern.
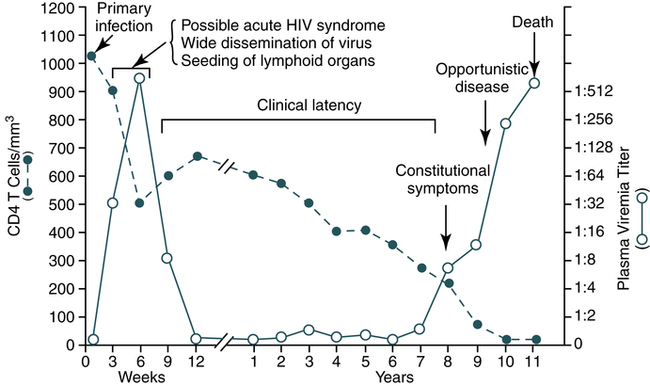
During the early period after primary infection, there is widespread dissemination of virus and a sharp decrease in the number of CD4 T cells in peripheral blood. An immune response to HIV ensues, with a decrease in detectable viremia followed by a prolonged period of clinical latency. The CD4 T cell count continues to decrease during the following years until it reaches a critical level below which there is a substantial risk of opportunistic diseases. (From Pantaleo G, Graziosi C, Fauci A: The immunopathogenesis of human immunodeficiency virus infection, N Engl J Med 328:327-335, 1993.)