A Series of Etiological Epidemiology Studies on Kaschin-Beck Disease (1965-1993)
A Series of Etiological Epidemiology Studies on Kaschin-Beck Disease (1965-1993)
Outline
Kaschin-Beck disease (KBD) is an endemic deforman Osteoarthrosis that mainly occurs in children. Patients with slight signs present symmetrical enlargement in finger, toe, knee, elbow and ankle joints, which may affect their labor ability. Those with serious signs having short limbs and fingers are dwarf with normal intelligence but lose their labor ability, leading disability in all lifetime.
This disease was found and first reported in 1849. The etiology study began in 1880s-1890s. Former Russian military doctor Kaschin and Beck were the pioneers in this area, and therefore it was call the Kachin-Beck disease. There had been more than 40 etiological hypotheses. However these could be summarized into 3 main hypotheses: 1) variation in amount of common or trace element in diet of endemic area; 2) organic pollution of drinking water; 3) poison of fusarium toxin in the grains of KBD area. The only common feature among these 3 hypotheses is that they all recognized the pathogenic agent that entered human body through the specific food in endemic area. However, what was pathogenic agent that was the mostly likely the cause? None of these hypotheses was confirmed and recognized by the public after frequent debates for many years due to many reasons. However, they were mainly coming from epidemiology study methods. They are: 1) the observation areas were too narrow and limited to represent the whole situation; 2) the observation time was not longer enough and the temporal relationship between the agent and this disease was not clear; and 3) the observation methods were not identical and standardized, which made it difficult to compare and identify the common agents.
It is difficult to reason and clarify the etiological and epidemiological problem of KBD. In the view of the “pure objective position”, looking at some of listed reports will result in a mess, just like entering the clouds. But with an attempt to confirm one kind of ideas, one would also easily jump to the conclusion with mistakes or bias. Therefore, the authors chose to present only the facts without making any further inference. This may make the readers to think what the facts lead us to. Except for a few intervention studies or laboratory animal studies, others were mainly typical investigations using historical prospective studies.
Up to the date this chapter was written, the authors had been studying KBD for 28 years since 1965. Having lived and worked in endemic areas for many years with colleagues, the authors had many interesting observations. What occurred repeatedly serve to verify the objective facts themselves. Based on request of the editor-in-chief editor of this book, some of documented research cases was abstracted and described in temporal order as follows.
1. Field observation in KBD areas
1.1 Survey at Yuanbao Village, Shangzhi County of Heilongjiang Province in September of 1965
Shangzhi County is located in the east mountain area of Heilongjiang and was the active and severe areas of KBD at that time. Yuanbao village, a remote rural area located 30 Kilometers east of Shangzhi Town, was a well-known severe KBD area of Shangzhi County, where Han and Korea nationality residents lived, with a total population of 2300 (2123 and 177 for Han and Korea, respectively). The accommodation situation for Han and Korea people were the same. They lived in the same kinds of house with different rooms or in houses next to each other and drunk the water from the same wells. Han people planted glebe and their mainly staple food was maize, whereas Korea people planted paddy field and their staple food was rice. The survey was conducted by a survey group of 3 doctors who surveyed the subjects from door to door and performed physical examinations for the house members. The Han people were sampled with a simple machine random method based on the order number of Hukou book (registered permanent residence book) for a proportion of 5:1 from a total of 426 persons (except single household), whereas Korea people were obtained from the census of a total of 177 persons. The survey was finished in a week, and the results are presented in Table 6.1.
Although the prevalence in Korea people was much lower than what had been perceived, the authors were very surprised by the real survey results due to a “huge difference”. This implied that that the Han people may have suffered severely from the pathogenic agent for KBD, whereas the Korea people were basically either lightly or completely not influenced by whatever the causes were.
Table 6.1 KBD at Yuanbao Village, Shangzhi County of Heilongjiang Province
Nationality
Total no. of persons
Patients
Prevalence (%)
Han
426
145
34.0
Korea
177
2
1.1
(Cited from ref.2)
1.2 Differences in living conditions between Han and Korea people inhabited in minority-mixed areas in Shangzhi County, Heilongjiang Province.
In October 1965, the authors invited 3 Han and 3 Korea intelligent farmers who were more than 50 years old to discuss the main differences in living styles between Han and Korea people in their villages. The question was “Due to some big differences in KBD prevalences between Han and Korea people, please think about which possible life-style factors may be related to this disease”. The life-style factors were meant to be any possible living conditions. The farmers were interviewed without any suggestions. After a 3-4 hour discussion, 4 common opinions were revealed: 1) Han people planted glebes and their staple food was maize, whereas Korea people planted paddy field and their staple food was rice; 2) There was few red pepper in the diet of Han people, but there were a lot red pepper in the diet of Korea people; 3) Korea people drank more alcohol than Han people; 4) Korea people were more healthy than Han people.
The 4 common opinions meant much more to the researchers. At that time, there was almost a common acceptable opinion by the academia and the public of the KBD areas that the occurrence of KBD was due to poor quality of water. However, these opinions were different from the existed one. At least at Yuanbao Village, there was no valuable difference in drinking water between Han and Korea people.
In the survey continued, from the original hypotheses provided by the common people, the researcher formulated some unique life characteristics: the 1st and 2nd opinions about Korea people were objective facts and need further observations. About drinking alcohol of the 3rd, adult and elder Korea people drank more alcohol but children did not. However, the occurrence of KBD mainly centralized in 5-12 years old children and adolescents. Therefore, drinking alcohol needed no further consideration. As for the 4th opinion, it had been reported previously that the prevalence of KBD in Han and Korea people was the same in some KBD areas. Therefore, it would not exist. Under this situation, a specific survey on KBD of Korea people was conducted to find out what characteristics of the Korea cases were possibly associated with the above first 2 opinions. The survey was conducted in the areas east of Shangzhi County between Oct. and Dec. 1965.
Case report of Korea KBD in east Shangzhi County (between October and December 1965)
The mountain area in the east of Shangzhi County had abundant water resource where Korea people lived and planted paddy field. Among the Korea people who planted paddy field, few of KBD cases occurred. Among 3 communities, 5 Korea production brigade and a small production brigade mixed with the Han production brigade, 38 patients with degree 1 KBD or more severe were found through door-to-door interviews and physical examinations. For each case, the following questions were asked: 1) How old was he/she when the diseases occurred? 2) Where did he/she live when this disease occurred? 3) Did they plant plebe or paddy field at that time? 4) What was their staple food at that time? In the end, 8 of the 39 cases could not remember the history of disease and could not answered these questions. The age ranged from 18 to 72 for the remaining 30 patients. Their diseases occurred when they were young and planted plebe, and their staple food was maize. The results are presented in Table 6.2.
Table 6.2 The staple food of maize, subsidiary food of hot pepper situation for the Korea patients before KBD occurred
Enjoy eating red pepper
Not enjoy eating red pepper
Total
No. of maize as staple food
25
1
26
No. of maize as most of diet
3
0
3
No. of rice more than maize as staple food
1
0
1
29
1
30
(Cited from ref. 2)
The conclusions of this survey were: 1) Twenty of 30 Korea people had KBD when they ate maize as the staple food; 2) only 1 of the 30 patient did not like eating red pepper. Obviously, those Korea who ate rice as the staple food did not suffer from KBD. All the cases occurred when they planted plebe and ate maize as the staple food. There was no association between eating red pepper and occurring of this disease.
1.3 Association between KBD occurrence and the Han people planting paddy field and eating rice as their staple food in the KBD area
The survey on KBD in Shengli Community, Wuchang County of Heilongjiang in July 1970: Shengli Community was well-known for severe KBD occurring in this area in history. It is located in the drainage areas of Mangniu River with an abundance of water resources. It was liberated from the old government in 1945, established the democratic government in 1946, carried out agriculture cooperation in 1955 and then rebuilt the plebe to paddy field in 10 years. Until 1970, most of production brigades had at least half of their total farmland rebuilt into paddy field. In some of the brigades, paddy field accounted 90% of their farmland, and only few brigades located in high topography still planted plebe.
In the survey, we selected 3 connected production brigades and surveyed from door-to-door and face-to- face. More than half the peasants in 2 of the production brigades in Shangyuan planted paddy field and ate rice as their staple food. Peasants in another production brigade Shuangshan planted plebe and 70.9% ate maize as their staple food. The results are presented in Table 6.3.
Conclusions: there was no patients under 20 years old in the production brigade which rebuilt plebe into paddy field. Meanwhile 13 of 65 under 20 years old suffered KBD in the control area where there was no plebe rebuilt into paddy field. Among people over 20 years old, the prevalence was 83/180 and 27/77 in paddy field and plebe production brigades, respectively. Both the brigades were of severe KBD areas. It was obvious that those adult patients contracted the disease when they planted plebe and ate maize as their staple food.
Table 6.3 The prevalence of KBD in the peasants in 2 paddy and 1 plebe field production brigades
Paddy field of Shengyuan
Plebe field of Shuangshan
Population
No. of Patients
Population
No. of Patients
Under 20
188
0
65
13
Above 20
180
83
77
27
368
83
142
40
(Cited from ref. 2)
1.4 Survey on Xincun Production Brigade, Hongwei Community, Baoshan Mineral area of Shuangyashan City (October 1970)
In 1963, Baoshan Mineral area of Shuangyashan city retrenched some of staff to establish several production brigades, one of which was Xincun production brigade. Xincun production brigade was set up in 1964, located in the inner of Baoshan Mineral Block, drank tap water as city inhabitants did, the food was provided partly by themselves between 1965 and 1966. Since 1967 all the food were provided by themselves. The Mineral area took care of and supported by-work production. By then the living standard was almost the same as what they had before they were retrenched. In the spring of 1970, KBD was found, and this survey was conducted in Oct. 1970. The students in the school were examined. As the controls, the students of worker households’ in school were also examined. The results are presented in Table 6.4.
Table 6.4 KBD examination on students in school in Xincun production brigade of Shuangyanshan city
Clinical examination
X-ray examination
Total No.
No. of patient
Prevalence (%)
Total No.
No. of patient
Prevalence (%)
Peasantry household
125
55
44.0
149
113
75.8
Worker household
118
1
0.8
87
4
4.6
(Cited from ref.2)
Originally, there was no KBD in the blocks in Baoshan Mineral area. At beginning of the establishment of Xinchun production brigade, there was no such disease. After 2 years of supporting food by the residents themselves, the KBD broke out. The peasantry households and worker households lived in the same blocks, drunk the same kinds of tap water provide by the town. Their living habits and conditions were similar. The only difference was that the staple food of peasantry households was maize planted by themselves and the staple food of worker households was maize provided by grain depot. From the temporal relationship, the emerging of a great deal of patients was 2-3 years after the peasantry ate the maize planted by themselves.
After carefully searching for the clues, it was found that a lot of similar cases existed.
1.5 Survey on KBD in the 3rd Production Brigade of Hushan, Linkou Country of Heilongjiang (March 1972)
The 3rd production brigade of Hushan, lying near the railway of Mudanjiang and Jianmusi City connected with the residence area of Hushan railway staff. There were 301 persons in the 3rd production brigade of Hushan. Excluding those lived there no long than 1year and those under 1 year, 43 households with 164 persons were surveyed. As the controls, 27 railway households with 108 persons were surveyed. The living standards between peasantry and railway households were similar, with the peasantry households slightly higher. Average salary for railway staff was 50 yuan per-month, with no more than 10 yuan /person/month in the household. Every labor person for peasantry household was 1.5-2.0 yuan/day. Peasantry household consumed more other foods such as vegetables and meat. Both the peasantry and worker households drank the running tower water that also was used for the trains. Therefore, drinking water was the same. People in the 3rd production brigade of Husan mainly ate maize planted by themselves. Railway staff bought maize from grain depot in the town. The result was that the prevalence of degree I and more severe KBD in peasantry household population was 26/164 but only 0/108 in railway staff households.
1.6 The survey on the prevalence of KBD in railway staff’s offsprings in Nenjiang Town, Qiqihaer Railway Station (1980).
In the east part of Heilongjiang province, people in the KBD areas ate maize as their staple food. Employees lived in the same area with peasants did not suffered from this disease. In the west part of Heilongjiang, people in KBD area ate wheat flour as their staple food. Some employees of town in KBD area suffered from this disease. The occurrence of KBD in employees in town was even more than that in the peasants lived in the same place. The results of survey on Nenjiang Town, Nenjiang County are presented in Table 6.5.
Table 6.5 KBD in Children (6-15) in Nenjiang Town (1979)
Nenjiang town
No.
Detected rate of clinical examination (%)
Detected rate of X-way (%)
Metaphysis (%)
Employees of Railway Station
82
24.4
52.4
20.7
Peasants in 3rd group, Siji village
42
9.5
26.1
9.5
Dependents of garrison
43
2.3
4.7
4.6
(Cited from ref. 2)
Only gold members can continue reading. Log In or Register to continue
Aug 1, 2016 | Posted by drzezo in INFECTIOUS DISEASE | Comments Off on A Series of Etiological Epidemiology Studies on Kaschin-Beck Disease (1965-1993)
 Explore Route of Transmission for Kala-azar
Explore Route of Transmission for Kala-azar
 The discovery of a new Rotavirus that caused adult epidemic diarrhea in China in 1980’s
The discovery of a new Rotavirus that caused adult epidemic diarrhea in China in 1980’s
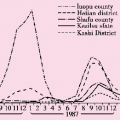 Epidemiological studies on a HEV epidemic in Xijiang province between 1986 and 1988
Epidemiological studies on a HEV epidemic in Xijiang province between 1986 and 1988
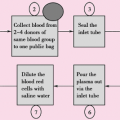 Discovery and Control of the HIV/AIDS Epidemic among Plasma Donors in China
Discovery and Control of the HIV/AIDS Epidemic among Plasma Donors in China
 The risk factors and mechanisms of hepatitis B virus intrauterine transmission
The risk factors and mechanisms of hepatitis B virus intrauterine transmission



