Fig. 26.1
(a) Iodine-123 scan (1.2 mCi; 444 MBq) indicating little detectable uptake. (b) Iodine-124 PET/CT (1.7 mCi;63 MBq) revealing a focus of uptake posteriorly
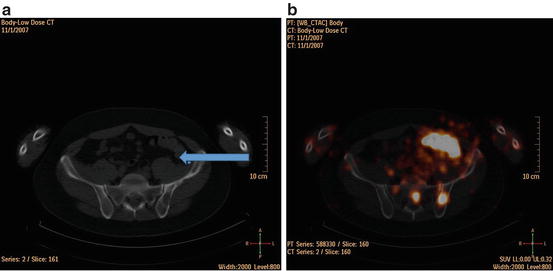
Fig. 26.2
(a) Computerized tomographic scan of pelvis indicating that the focus positive on PET scan was located in the left pelvic bone (arrow). (b) Fusion of the transverse CT image of the pelvis with the corresponding transverse iodine-124 PET image demonstrating localization of the lesion. The fused images demonstrated that the abnormal iodine-124 uptake corresponded precisely to the abnormality on the CT scan. In addition to localizing this abnormality, the 124I images demonstrated a second focus of abnormal iodine-124 uptake that correlated with another abnormality in the sacrum on the CT image suggesting an additional metastasis
Clinical Pearls/Pitfalls
1.
It is useful to tailor therapeutic interventions by risk stratification of patients according to 2014 ATA Guidelines on outcome status after initial treatment, which in this case indicated a biochemically incomplete response that was subsequently shown after iodine-124 PET scanning to be structurally incomplete.
2.
Iodine-124 is associated with improved imaging over iodine-123 and lower radiation dose than iodine-131, thereby avoiding stunning. Although iodine-124 availability is currently confined to larger academic centers (because it is not an FDA-approved radioisotope and an IND is required), iodine-124 PET/CT scan should be considered in patients in whom the serum Tg is elevated to >10 ng/ml and the traditional iodine-131 scan is negative.
3.
Another difference between iodine-124 and iodine-123 or iodine-131 is that iodine-124 emits a positron and can be imaged with a positron emission tomography (PET) scanner. The positron-emitting iodine-124 in combination with PET/CT makes it possible to measure the spatial distribution of radioiodine in tumors and normal organs at high resolution and sensitivity. Thus, iodine-124 PET/CT may provide improved delineation of the extent of metastases in well-differentiated thyroid cancer.
4.
Radioiodine refractory tumors or those that fail to take up radioiodine should not be given additional doses of iodine-131.
References
1.
Haugen BR, Alexander EK, Bible KC, Doherty GM, Mandel SJ, Nikiforov Y, et al. American Thyroid Association Management Guidelines for patients with thyroid nodules and differentiated thyroid cancer. Thyroid. 2015; 24.
2.
Marcus C, Whitworth PW, Surasi DS, Pai SI, Subramaniam RM. PET/CT in the management of thyroid cancers. Am J Roentgenol. 2014;202(6):1316–29.CrossRef
3.
Riemann B, Uhrhan K, Dietlein M, Schmidt D, Kuwert T, Dorn R, et al. Diagnostic value and therapeutic impact of (18)F-FDG-PET/CT in differentiated thyroid cancer. Results of a German multicentre study. Nucl Med. 2013;52(1):1–6.
4.
Leboulleux S, Schroeder PR, Schlumberger M, Ladenson PW. The role of PET in follow-up of patients treated for differentiated epithelial thyroid cancers. Nat Clin Pract Endocrinol Metab. 2007;3:112–21.CrossRefPubMed
Related posts:
 A Case of Multifocal Papillary Thyroid Microcarcinoma
A Patient with Papillary Thyroid Cancer and Biochemical Evidence of Disease at the One-Year Follow-Up Visit
A Case of Papillary Thyroid Cancer Without Aggressive Histological Features with Nodal Metastases in an Older Patient
RAI-Refractory, Advanced Differentiated Thyroid Cancer Receiving Tyrosine Kinase Inhibitor Treatment: Checking for Drug-Drug Interactions
A Case of Multifocal Papillary Thyroid Microcarcinoma
A Patient with Papillary Thyroid Cancer and Biochemical Evidence of Disease at the One-Year Follow-Up Visit
A Case of Papillary Thyroid Cancer Without Aggressive Histological Features with Nodal Metastases in an Older Patient
RAI-Refractory, Advanced Differentiated Thyroid Cancer Receiving Tyrosine Kinase Inhibitor Treatment: Checking for Drug-Drug Interactions
 A Child with Papillary Thyroid Cancer and Locally Advanced Disease but No Distant Metastasis
A Child with Papillary Thyroid Cancer and Locally Advanced Disease but No Distant Metastasis
 Timing and Extent of Surgery for a Pediatric Patient with Hereditary MTC and Positive Screening for the S891A RET Mutation
Timing and Extent of Surgery for a Pediatric Patient with Hereditary MTC and Positive Screening for the S891A RET Mutation
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


