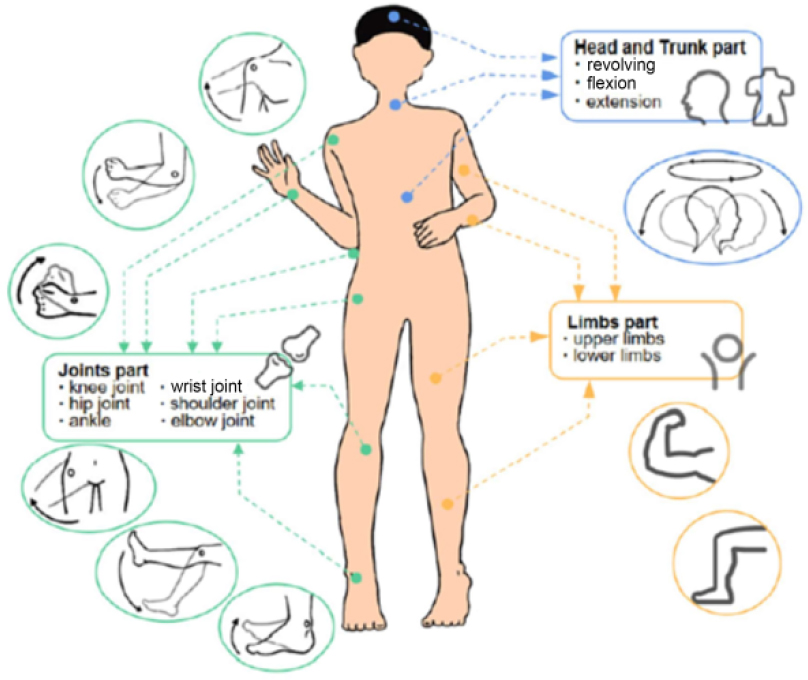
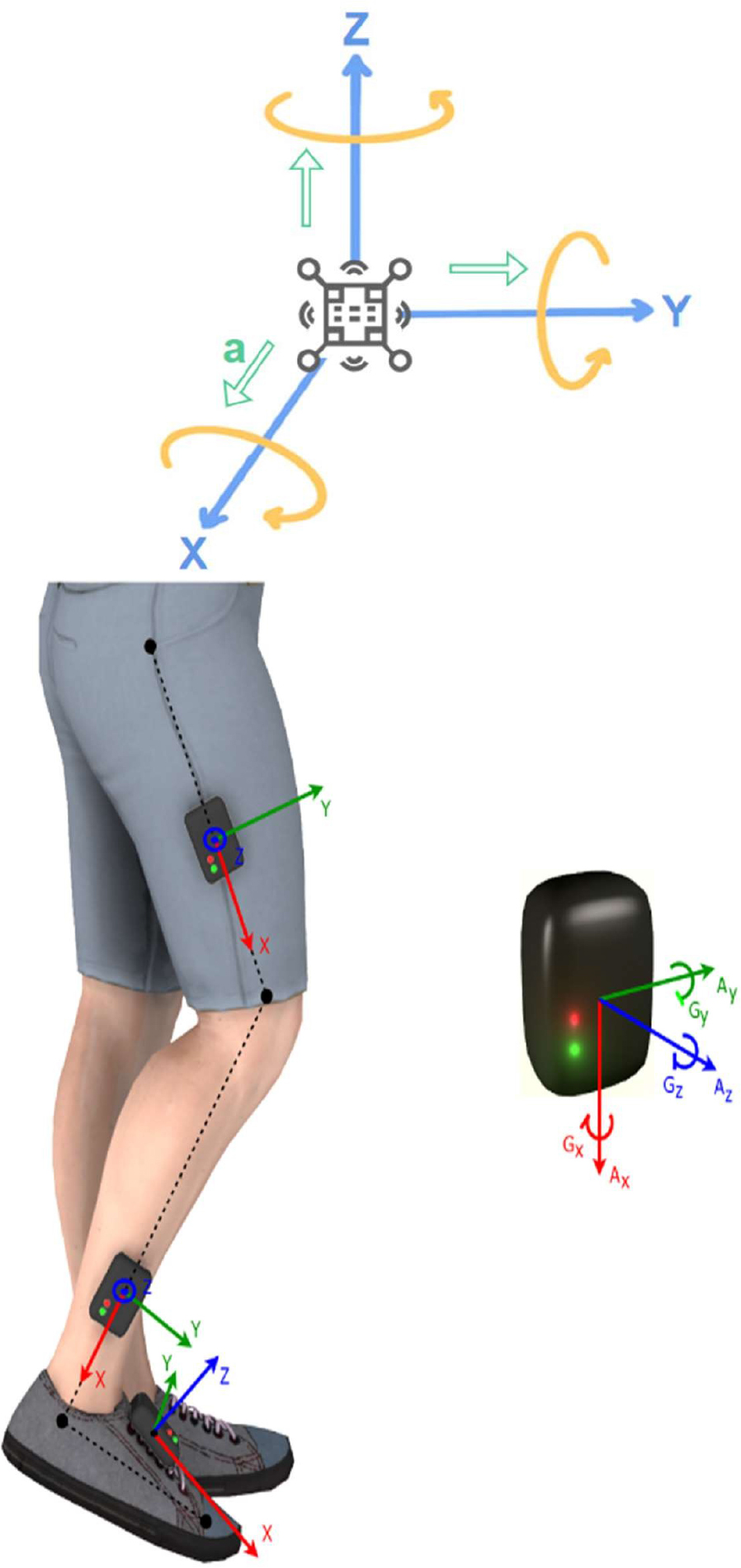
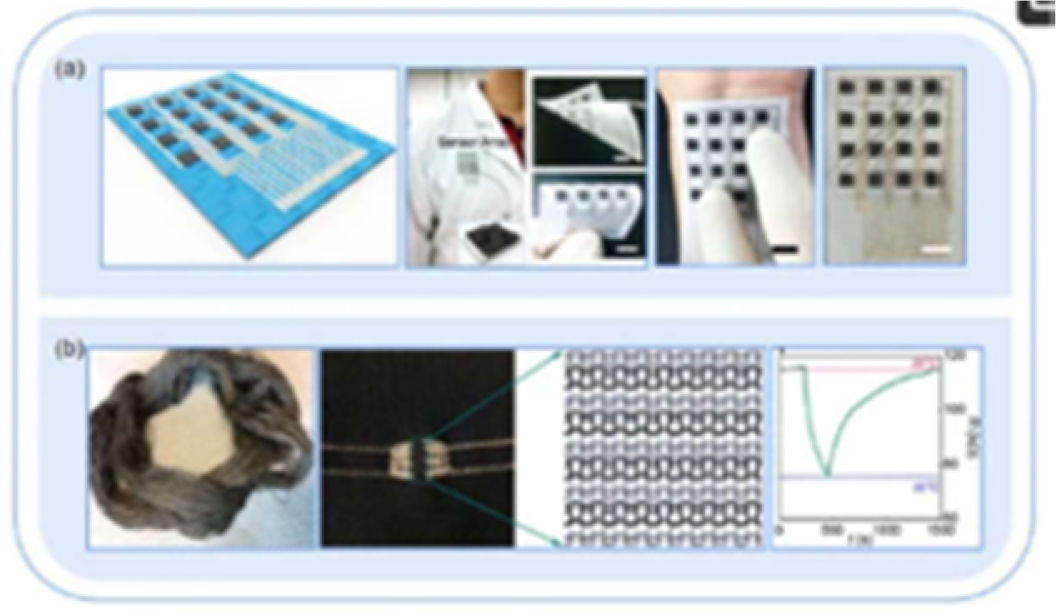
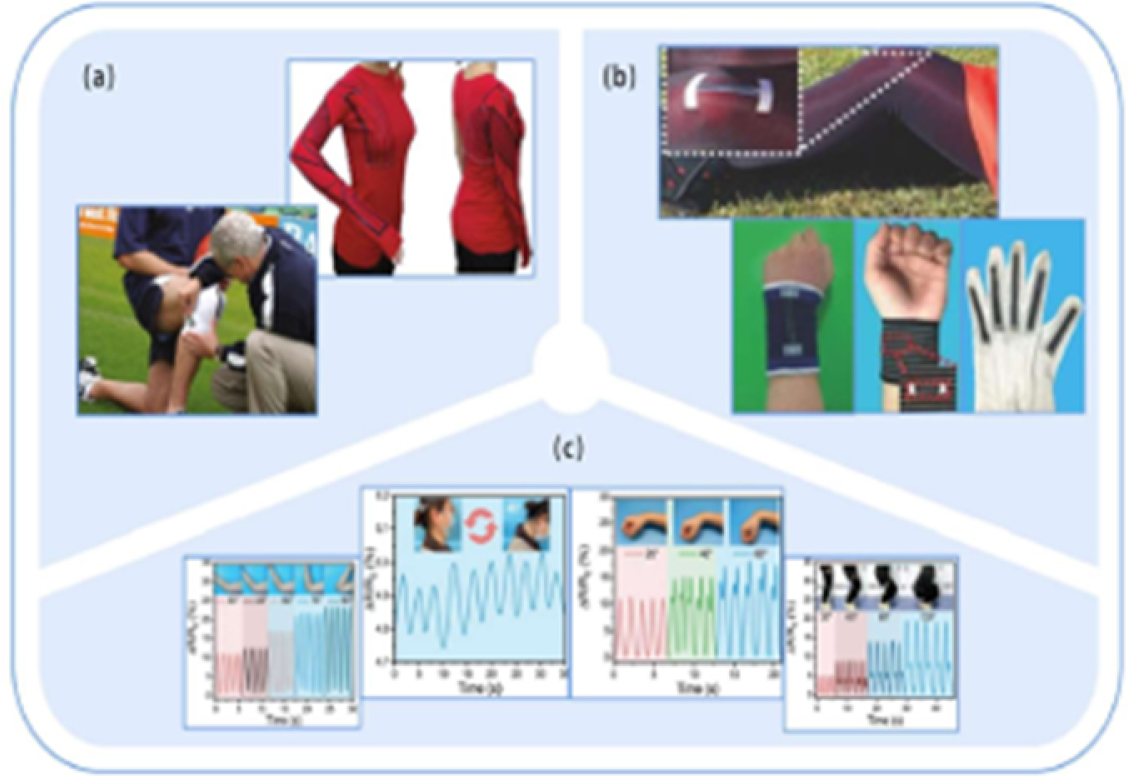
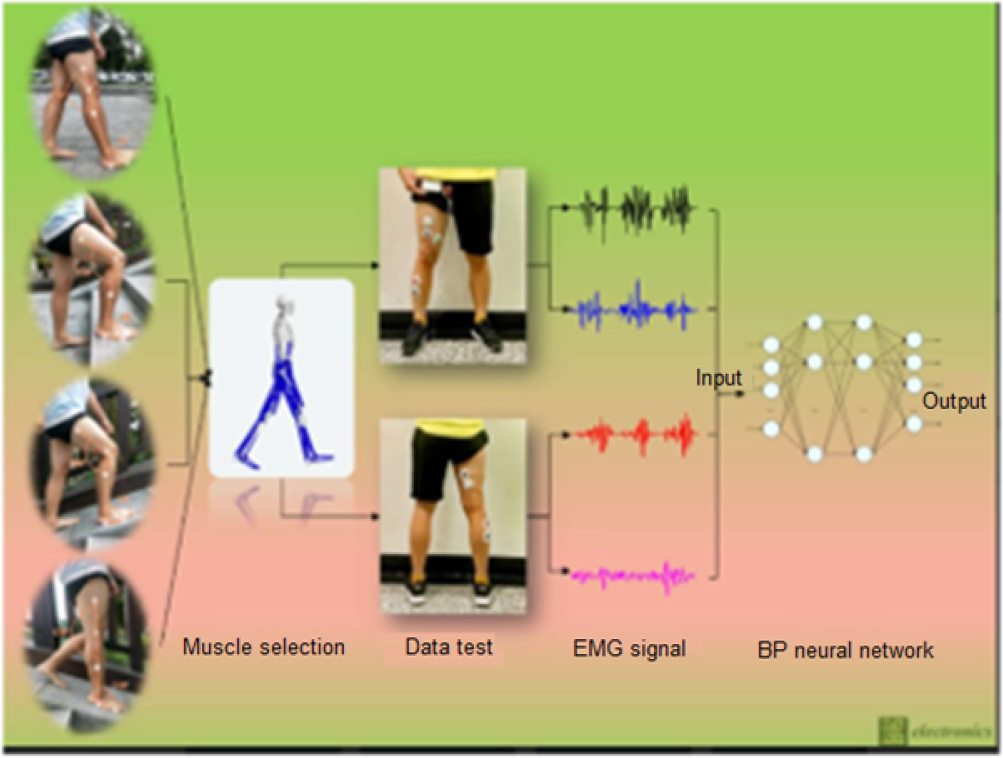
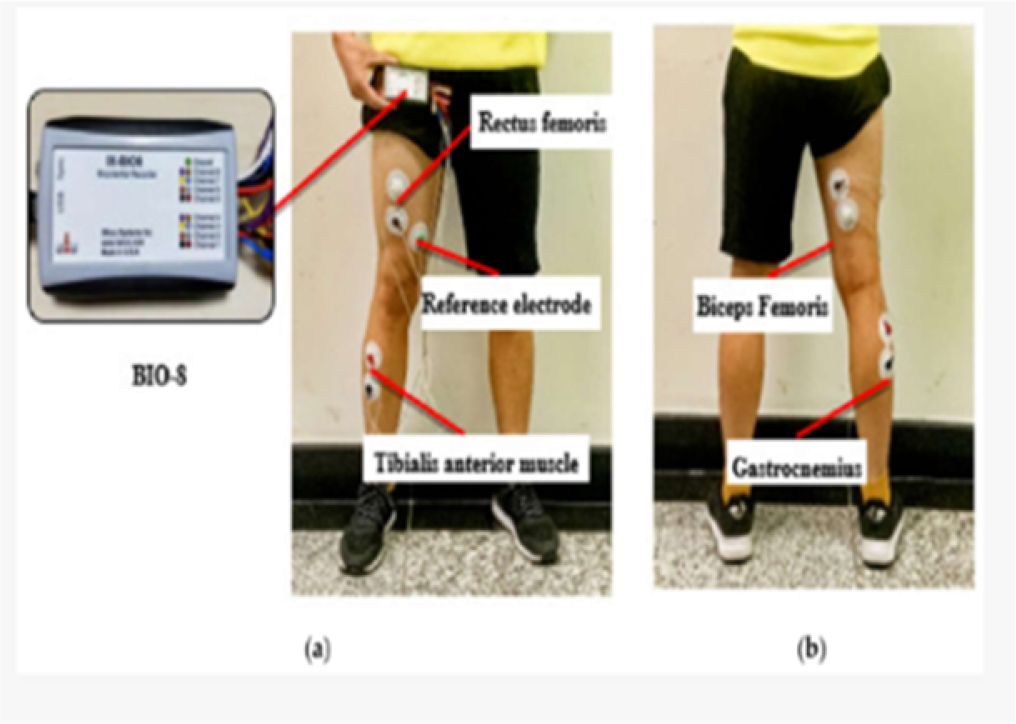
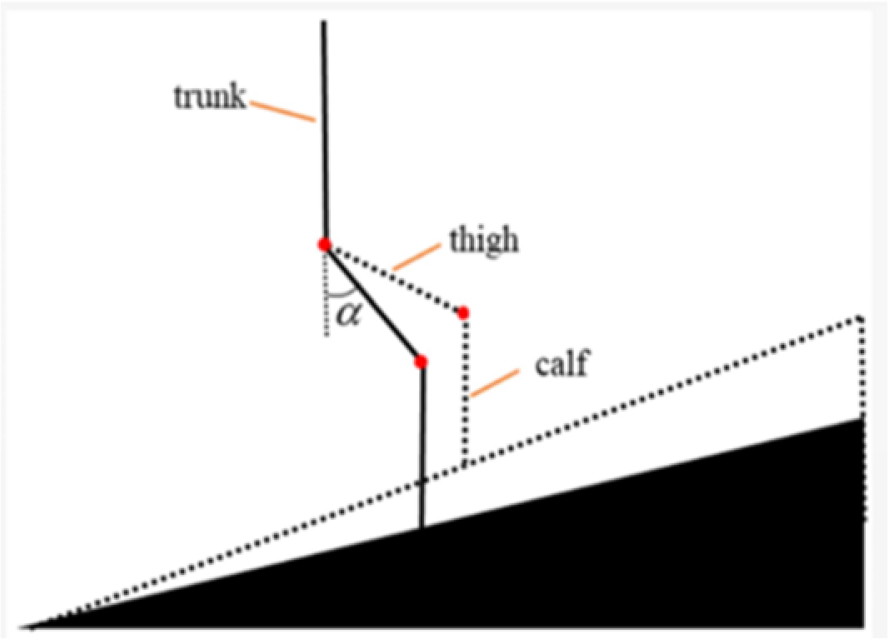
The integration of biomedical sensors into physiotherapy has revolutionized the assessment and rehabilitation of human movement. These sensors, both invasive and noninvasive, measure critical biomechanical parameters such as force, pressure and motion, enabling physiotherapists to conduct accurate diagnostics and monitor rehabilitation progress. Traditional silicon-based sensors such as accelerometers, gyroscopes and magnetometers form the backbone of wearable technologies, enabling real-time tracking of body movement. Complementing these are flexible sensors, including textile-based strain and pressure sensors, offering superior comfort and adaptability for patients. The chapter also explores biophysical measurements, emphasizing the role of force and pressure sensors in evaluating muscle strength, joint stability and gait dynamics. Modern physiotherapy uses advanced tools such as digital goniometers, tilt sensors and inertial measurement units (IMUs) for comprehensive joint mobility assessments. Additionally, artificial intelligence (AI) is being integrated with sensor technologies to enhance rehabilitation outcomes. AI enables predictive analysis, personalized treatment planning and real-time biofeedback, thereby improving patient motivation and safety. The synergy between AI and sensor data facilitates early detection of abnormalities, risk prevention and continuous remote monitoring. Together, these innovations ensure precision-driven, patient-centered physiotherapy interventions. This chapter underscores the importance of ongoing research and technological advancement in developing smarter, safer and more efficient rehabilitation tools tailored to individual patient needs. Physiotherapy research frequently uses biomedical sensors to measure a variety of biomechanical factors. Often, they are called biomedical transducers and are the main building blocks of diagnostic medical instrumentation found in physiotherapists’ and biomedical engineers’ laboratories (Jones 2010). The need for accurate medical diagnostic procedures places stringent requirements on the design and use of biomedical sensors (Jones 2010). Usually, the first step in developing a biomedical sensor is to access the accuracy, sensor operating range, response time, sensitivity, resolution and reproducibility of the sensor. Once the need of the device is met, it becomes easy to choose among various available sensors and ensure that the measurement remains sensitive, stable, safe and cost-effective (Enderle and Bronzino 2012). Sensors also provide a non-hindrance assessment of human kinematic motion and motion status during exercise training or during rehabilitation. Nevertheless, there is a significant lack of studies on motion monitoring index systems, comprising rigid and/or flexible sensors, with a well-designed wearable system along with different angles of joint motion, especially for gross trunk mobility, complex joint movements and limb movements (Jones 2010; Enderle and Bronzino 2012). Depending on their particular applications, sensors are usually categorized as physical, electrical or chemical based on the quantity to be measured (Jones 2010). Biosensors are a special subclassification of sensors that have two distinct components: The transducer’s function is to convert the mechanical reaction into visual, electrical or physical signals proportional to the concentration of particular biomechanics (Enderle and Bronzino 2012). Both invasive and noninvasive sensors used by biomedical engineers will be covered in this chapter. Physiotherapy and rehabilitation can make use of a variety of mechanical sensors. Every sensor serves a distinct purpose, either supporting or carrying out the biomechanical processes of the human body. Physiotherapy equipment, investigative or therapy related, is mostly noninvasive with the sensor being attached to the external body part. Thus, sensors can be classified into several categories (Bowman and Meindl 1986; Mendelson 2005; Jones 2010; Enderle and Bronzino 2012): Whenever the sensor comes into contact with body fluids, the host itself may affect the sensor’s function, or the sensor may affect the site in which it is implanted. Hence, the materials used in the construction of the sensor’s outer body must be non-thrombogenic and nontoxic since they play a critical role in determining the overall performance and longevity of an implantable sensor (Bowman and Meindl 1986; Sani et al. 2021). According to Huang et al. (2023) motion monitoring sensors can be classified on the basis of: Physiological signals, such as electromyography (EMG) and electrocardiography (ECG), can also identify muscle contractions and heart contractions, the latter of which is a muscle. They do, however, function as a less accurate indirect method for gross motor training, particularly when it comes to electromyography. Recent developments in EMG have suggested the use of needle electrodes, which provide a detailed analysis of the fiber recruitment method. However, it becomes challenging to use the voltage and frequency patterns of muscle activity to determine the precise motion amplitude or angle, particularly in a 3D gross motor assessment. Accelerometers use their electrical impulses to identify deflection or stress variances from external acceleration. Gait monitoring, human motion analysis, fall detection and energy consumption estimation are all common uses for these. Three-axial accelerometers, which have an accuracy of ± 2 g and a sampling rate of 50–100 Hz, are currently commonly used. These days, most wearable systems are made up of triaxial accelerometers, which are frequently positioned on the body’s moving parts, such as joints and limbs (Huang et al. 2023). Figure 11.1. Diagram of an accelerometer showing its components and basic working principle Figure 11.2. Two basic types of accelerometers commonly used in prototype builds The above images are two basic types of accelerometers commonly used in prototype builds (Niu et al. 2018). Figure 11.3. Example of a gyroscope sensor for measuring angular variance in human motion Figure 11.4. Schematic of a magnetometer used for detecting orientation based on Earth’s magnetic field Figure 11.5. An inertial measurement unit (IMU) combining accelerometer, gyroscope and magnetometer sensors Excellent stretchability, biocompatibility, good compliance and high sensitivity are all included in them. The flexible sensor is used for augmented and virtual reality, human–computer interaction and human mobility monitoring and can be separated into two main groups: thin-film sensors and textile sensors, both of which have pressure and strain sensors (Huang et al. 2023). Figure 11.6. Example of flexible textile-based sensors integrated into daily-use garments (Huang et al. 2023) Current research suggests that strain sensors are commonly used to detect changes in the body’s position and for kinesthetic monitoring (Huang et al. 2023). Pressure sensors translate the pressure into an electrical signal, in contrast to strain sensors. They can be used extensively to detect finger motion, including pressure, twisting, extension and flexion force, and they have a detecting capacity of above 10 kPa. Joint motion recognition is another application for these sensors. These are now used for plantar pressure distribution during stance and gait monitoring. They are further illustrated in Figures 11.7 and 11.8 (Huang et al. 2023). Figure 11.7. Diagram of a flexible strain sensor translating mechanical deformation into electrical signals Figure 11.8. Diagram of a flexible pressure sensor for detecting applied force and pressure distribution These measurements study specific functions which change over time. These changes can yield significant statistical data, which can be used to determine the effectiveness of the therapy or assist in diagnosis. Biophysics is defined as “the physical and mechanical properties of the cells/tissues which can be used to either assess or modify functioning of the cells/tissues and can be studied in detail” (Jones 2010). Some examples of biophysical measurements in physiotherapy include: Table 11.1. Components of electrotherapy modalities and their functions in physiotherapy Noninvasive sensors are most commonly used in physiotherapy. The biopotential measurements required in physiotherapy are as follows: force measurement (load or weight); muscular force measurement; joint movement measurement; fascia pliability measurement; response or reaction time measurement. A few sensors along with their biomechanical measurements and uses are mentioned below. Yet, there are many biomechanical functions which can be developed or are under-development, necessitating further studies. Force measurement is crucial for physiotherapists as it provides objective data to assess muscle strength, joint function and biomechanical performance during rehabilitation. By measuring the force exerted during exercises, physiotherapists can track a patient’s progress, ensure safe load-bearing and adjust rehabilitation plans accordingly. Force measurement helps prevent re-injury by avoiding overloading or underloading the affected area, guiding exercise progression and ensuring the rehabilitation process is tailored to the patient’s specific needs, promoting optimal recovery and functional outcomes. Force measurement during gait is crucial in physiotherapy as it helps assess how weight is distributed across the joints and muscles while walking. This data enables physiotherapists to identify movement abnormalities, such as uneven load-bearing or muscle weakness, and tailor rehabilitation programs to address these issues. By monitoring gait forces, therapists can ensure more effective recovery and prevent re-injury, promoting better mobility and overall function. Biomechanically, gait is classified into two major phases: swing and stance phases. The stance phase is where the lower extremity touches the ground and the swing phase is where the lower extremity is off the ground. The main biomechanical analysis of gait in either phase is: Thus, as stated, the area of weight bearing is given more importance in stance phase than swing. The quantitative measurement of the amount of force induced by the muscle during stance and swing phases varies as the movements of the joint differ. Thus, quantitative assessment becomes equally important along with qualitative muscle recruitment strategy. Thus, muscular force measurement becomes important in gait. An example of sensors which detect the muscular force during static posture or dynamic movements is electromyography sensors. Electromyography is a device which uses electrodes to pick up electrical signals from the muscle during its contraction and sends the impulse to the machine. The machine records the signals in detail and projects the information in graph form as an electromyograph. The signals are detected by the electrical pads placed on the area of contact through a velcro strap. Aqua Gel is placed between the electrode and the skin in order to reduce artifaction. Hence, these electric pads are called EMG sensors. Muscular contraction generates an electrical signal, or EMG signal, that can be detected by the EMG sensor. The recordings vary according to the phases of EMG. Figure 11.9 shows the diagrammatic representation (Wang et al. 2021). Figure 11.9. Electromyography (EMG) signal patterns during different muscle contraction phases (Wang et al. 2021) Figures 11.10–11.12 demonstrate the position of the selected muscle and the reference electrodes (Wang et al. 2021). Figure 11.10. Positioning of selected muscle and placement of reference electrodes for EMG measurement Figure 11.11. Placement of EMG electrodes for upper or lower limb muscle activity detection Figure 11.12. Example of EMG electrode placement for gait analysis Because they provide precise, real-time data that aids physicians in evaluating, tracking and optimizing the recovery process, force measurement sensors are essential to physiotherapy. Both the patient and the physiotherapist can benefit from these sensors’ ability to monitor the force or pressure used during particular movements or exercises. They support physiotherapy in the following ways: Pressure measurement in physiotherapy is essential for assessing and optimizing a patient’s biomechanical performance during rehabilitation. By measuring pressure distribution across the body, such as under the feet, back or other body parts, it means physiotherapists can analyze how forces are transmitted through the body during movements such as standing, walking or exercising. This helps identify areas of excessive pressure or insufficient load-bearing, which can indicate improper posture, misalignment or muscle imbalances. For example, an uneven distribution of pressure across the feet may suggest gait abnormalities, while concentrated pressure on certain body parts can indicate incorrect posture or compensation patterns. Real-time feedback from pressure sensors helps patients adjust their movement patterns, ensuring that forces are applied efficiently, minimizing the risk of injury and improving overall biomechanics (Patel and Patel 2020). Pressure data also assists in tracking the progress of joint mobility or strength after injury or surgery, providing insight into how the body is adapting to stress over time. In cases of conditions such as stroke, arthritis or paralysis, pressure measurement can help identify areas at risk for pressure ulcers or sores, prompting early interventions to prevent such injuries. By enabling precise, data-driven adjustments to rehabilitation programs, pressure measurement helps improve movement efficiency, stability and comfort, ultimately promoting safer and more effective recovery.
11
AI-driven Sensor Technologies in Physiotherapy and Oncology: Transforming Rehabilitation Through Intelligent Biomechanical Monitoring
11.1. Introduction
11.1.1. Sensor classification
11.1.2. Sensor packaging
11.2. Sensors for monitoring human motion
11.2.1. Traditional silicon-based sensors


11.2.2. Flexible sensors

11.3. Biophysical measurements in physiotherapy
Parts
Function
Modality
Generates the current in required frequency.
Cables
Pass the current from the modality/system to the electrode (the contacting part of the machine to the body).
Electrodes
These are commonly made up of rubber or metal in order to conduct the electric current from the machine to the part in contact.
Aqua Gel
Decreases the resistance between the electrode and the skin so that the current passes smoothly.
11.3.1. Force measurement
11.3.1.1. Working principles (Zheng et al. 2022)
11.3.1.2. Role of force measurement sensors in physiotherapy
11.3.1.3. Artificial intelligence integration in force measurements
11.3.2. Pressure measurement
Related posts:
 AI-driven Imaging in Oncology and Physiotherapy: A Game-changer in Diagnostics
AI-enhanced Virtual Rehabilitation: The Future of Cancer Recovery
Integrating AI with Physiotherapy to Improve Quality of Life for Cancer Patients
Personalized AI-based Exercise Therapy for Oncology and Physiotherapy Patients
AI-driven Motion Analysis for Physiotherapy in Cancer Survivors
AI-driven Imaging in Oncology and Physiotherapy: A Game-changer in Diagnostics
AI-enhanced Virtual Rehabilitation: The Future of Cancer Recovery
Integrating AI with Physiotherapy to Improve Quality of Life for Cancer Patients
Personalized AI-based Exercise Therapy for Oncology and Physiotherapy Patients
AI-driven Motion Analysis for Physiotherapy in Cancer Survivors
 AI-driven Innovations in Biomaterial-based Physiotherapy and Oncology: Personalizing Patient Care Through Intelligent Monitoring and Predictive Rehabilitation
AI-driven Innovations in Biomaterial-based Physiotherapy and Oncology: Personalizing Patient Care Through Intelligent Monitoring and Predictive Rehabilitation
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


