Highlights
- •
The first to analyze data retrospectively from pediatric PTC patients in a large medical unit with a particular focus on LNM patterns.
- •
Comparative analysis between DSV-PTC and C-PTC focus on pediatric population for the first time.
- •
Explored the risk factors associated with LNM in C-PTC, providing valuable insights for clinical practice.
Abstract
Objective
To analyze the clinicopathological features and predictors of lymph node metastasis (LNM) in the diffuse sclerosing variant of papillary thyroid carcinoma (DSV-PTC) and compare these findings with conventional papillary thyroid carcinoma (C-PTC) in pediatric populations.
Methods
Patients aged 18 years or younger who were preoperatively diagnosed with PTC and underwent thyroidectomy at the First Affiliated Hospitals of Nanchang University from January 2017 to May 2024 were included in this study. Demographic and clinicopathological characteristics were retrospectively analyzed. Univariate and multivariate analyses were performed to identify risk factors for lymph node metastasis. Clinical outcomes, including nerve injury, hypocalcemia, and recurrence, were also recorded and evaluated.
Results
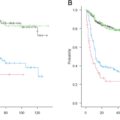
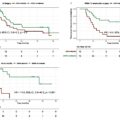
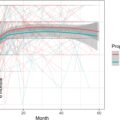
A total of 119 children were enrolled in this study, with a median age of 15.6 years. Of these, 89 (74.8 %) were female, and 18 (15.1 %) were diagnosed with DSV-PTC. Central lymph node metastasis (CLNM) was observed in 94 (79 %) patients, while 60 (50.4 %) had lateral lymph node metastasis (LLNM). DSV-PTC was associated with a higher incidence of CLNM and LLNM compared to C-PTC (p = 0.039, p < 0.001). Multifocality and bilateral tumors were also more common in DSV-PTC ( p < 0.001). Cox regression analysis identified tumor size as an independent predictive factor for CLNM in pediatric C-PTC patients. Tumor size, ETE and the presence of CLNM were independent predictive factors for LLNM. After a mean follow-up of 32.8 months, no patient died from the disease, but four C-PTC patients (4.0 %) developed local recurrences, which were managed surgically. Lung metastasis occurred in 2 (11.1 %)
DSV-PTC and 1(1.0 %)C-PTC patients, respectively. Permanent injuries included one case of unilateral recurrent laryngeal nerve(RLN) injury and two cases of bilateral RLN injury. Four patients (4.0 %) experienced temporary hypocalcemia, which resolved after 6 months of calcium therapy.
Conclusions
DSV-PTC presents unique characteristics of lymph node metastasis and may be more aggressive than conventional PTC in pediatric populations. The presence of CLNM, tumor size and ETE were identified as independent predictors of LLNM in pediatric patients with conventional PTC. Evaluating these prognostic factors may help in customizing individualized surgical approaches for children, thereby reducing unnecessary surgical complications.
Introduction
The prevalence of papillary thyroid carcinoma (PTC) in children varies widely, from 3 % to 70 % . Children with PTC are more likely to present with regional lymph node involvement, extrathyroidal extension (ETE), and distant metastasis . Despite the extensive disease at clinical presentation, children are much less likely to die from the disease compared to adults. The most common pathological type of thyroid cancer in children is PTC, which includes several histologic variants: classic, solid, follicular, and diffuse sclerosing .
The diffuse sclerosing variant of papillary thyroid carcinoma (DSV-PTC) is an uncommon and more aggressive variant of PTC. It is characterized by diffuse enlargement of the thyroid gland, heterogeneous hypoechogenicity, and diffuse scattered microcalcifications on ultrasonography . DSV-PTC presents with distinct clinical and pathological features, as compared to other thyroid cancers, including a higher frequency of cervical and pulmonary metastases at the time of diagnosis .
Currently, the patterns and predictors of neck spread in pediatric PTC, particularly across different pathological types, remain poorly understood. Much of the available data on indicators and treatment parameters are derived from adult populations, leading to ongoing debate about the necessity of complete thyroidectomy and lymph node dissection in pediatric PTC patients. Moreover, most studies reporting risk factors for lymph node metastasis (LNM) in pediatric PTC have not accounted for the influence of DSV-PTC .
This study described the patterns and predictors of LNM in pediatric PTC and compared the differences between DSV-PTC and conventional PTC (C-PTC) in the pediatric population. It also explored postoperative outcomes and common complications, aimed at determining the most appropriate management strategies. Our findings may contribute to the development of individualized surgical approaches, potentially minimizing unnecessary surgical complications in pediatric patients.
Materials and methods
Study population
We retrospectively analyzed the medical records of all PTC patients aged 18 years or younger at the First Affiliated Hospitals of Nanchang University between January 2017 and March 2024. The inclusion criteria for this study were: 1) aged 18 years or younger; 2) pathological diagnosis of PTC (classic, solid, follicular, and tall cell variants were grouped as C-PTC, diffuse sclerosing variant as DSV-PTC); 3) availability of complete medical records; and 4) patients who underwent thyroidectomy along with central lymph node dissection (CLND), with or without lateral lymph node dissection (LLND).
The exclusion criteria were: 1) age > 19 years; 2) postoperative pathology revealing another type of malignant thyroid tumor; 3) a history of thyroid surgery or laparoscopic thyroidectomy; and 4) incomplete medical records or missing follow-up data. A total of 119 patients met the inclusion criteria and were enrolled in this study. The study was approved by the Ethics Committee of the First Affiliated Hospital of Nanchang University. Data collection and analysis were conducted in accordance with institutional guidelines and the ethical standards of the Helsinki Declaration. The requirement for informed consent was waived due to the retrospective nature of the study.
Preoperative examination
All patients underwent high-resolution ultrasound and chest X-ray. Cervical contrast-enhanced computed tomography (CT) was not routinely performed and was reserved for cases with large or fixed thyroid masses, vocal cord paralysis, bulky metastatic lymphadenopathy, or distant metastasis. Preoperative ultrasound-guided fine-needle aspiration was conducted in all cases. Demographic and clinicopathological data, including gender, age, tumor size, tumor location, pathological type, Hashimoto’s thyroiditis (HT), focality (unifocal or multifocal), laterality (unilateral or bilateral), ETE, lymphovascular invasion, and pathological lymph node metastases, were retrospectively analyzed. All pathology specimens were microscopically examined and cross-checked by two or more experienced pathologists.
Surgical procedures
Intraoperative nerve monitoring (IONM) was routinely used in thyroidectomy (TriVantage EMG tube; Medtronic,USA). In our institution, intraoperative frozen section histology was performed for all tumors. Lobectomy plus isthmusectomy with ipsilateral CLND was performed for unilateral PTC. For patients with bilateral thyroid cancer or DSV, total thyroidectomy plus bilateral CLND was conducted. Total thyroidectomy plus bilateral CLND was also performed in cases where a nodule was detected in the isthmus or when the nodule size exceeded 4 cm. If lateral lymph node metastasis (LLNM) was suspected by the surgeon, evident on preoperative imaging, or confirmed by fine-needle aspiration cytology, a functional LLND was performed. Parathyroid gland reimplantation was routinely performed in cases of suspected parathyroid gland deficiency or hypovascularity.
CLND included the removal of the Delphian lymph node, the pretracheal lymph node, and the affected paratracheal lymph node, while bilateral CLND included the Delphian lymph nodes, pretracheal, and bilateral paratracheal lymph nodes. When functional LLND was required, the incision was extended to at least include lymph nodes at levels II–IV, level V was dissected when invaded. All surgeries were performed by high-volume surgeons with an annual thyroid surgery volume exceeding 1,000 cases.
Postoperative follow-up examinations were typically conducted at 1, 6, and 12 months, and every 6 months thereafter. Patients requiring calcium supplementation 6 months after surgery were diagnosed with permanent hypoparathyroidism. Recurrence was defined as local or regional disease after the initial surgery and was diagnosed via ultrasound-guided fine-needle aspiration cytology. Patients with distant metastasis or persistent disease were excluded from evaluation of recurrence.
Statistical analysis
Statistical analyses were performed using SPSS software, version 23.0. Continuous variables were expressed as mean ± standard deviation (SD), while categorical variables were reported as numbers and percentages. Differences were assessed using the chi-square test or Fisher’s exact test as appropriate for categorical variables. Non-parametric continuous variables were compared using Wilcoxon rank-sum test. Univariate analysis was performed using univariate logistic models, and variables with P values < 0.05 in the univariate analysis were further evaluated using multivariate logistic models. Multivariate analysis was conducted using binary logistic regression to identify independent risk factors for central LNM (CLNM) and lateral LNM(LLNM). Statistical significance was defined as P < 0.05.
Results
Patient characteristics
Between January 2019 and March 2024, 119 patients meeting the inclusion criteria for this study ( Table 1 ). The median age of the cohort was 15.6 years (range: 7–18), and 89 (74.8 %) were female. Of the 119 pediatric PTC patients, 18 (15.1 %) were diagnosed with DSV-PTC, with 17 (94.4 %) cases involving the entire gland lobe. The average tumor size was 2.31 ± 1.39 cm (mean ± SD), ranging from 0.35 to 5.70 cm. Lymphatic invasion was observed in only a few patients (9.2 %). ETE and multifocality were present in 33 (27.7 %) and 62 (52.1 %) patients, respectively. Bilateral lobe involvement was seen in 48 (40.3 %) patients, and 46 (38.7 %) had HT. CLNM was found in 94 (79.0 %) patients, and 59 (49.6 %) had LLNM.
| characteristics | ALL = 119 |
|---|---|
| Sex | |
| Male,N(%) | 30(25.2 %) |
| Female,N(%) | 89(74.8 %) |
| Age(yrs),mean(SD)[range] | 15.60(2.74) |
| <11,N(%) | 6(5.0 %) |
| 11–18,N(%) | 113(95.0 %) |
| Manifestations | |
| Neck mass | 91(76.5 %) |
| No symptoms | 28(23.5 %) |
| HT | |
| Yes,N(%) | 46(38.7 %) |
| No,N(%) | 73(61.3 %) |
| Multifocal tumor | |
| Yes,N(%) | 62(52.1 %) |
| No,N(%) | 57(47.9 %) |
| Bilateral tumor | |
| Yes,N(%) | 48(40.3 %) |
| No,N(%) | 71(59.7 %) |
| Size(cm),mean(SD)[range] | 2.31(1.39)[0.35–5.70] |
| ETE | |
| Yes,N(%) | 33(27.7 %) |
| No,N(%) | 86(72.3 %) |
| CND | |
| ipsilateral | 59(49.6 %) |
| bilateral | 60(50.4 %) |
| LND | |
| ipslateral | 42(35.3 %) |
| bilateral | 19(16.0 %) |
| none | 58(48.7 %) |
| CLNM | |
| Yes,N(%) | 94(79.0 %) |
| No,N(%) | 25(21.0 %) |
| LLNM | |
| Yes,N(%) | 60(50.4 %) |
| No,N(%) | 59(49.6 %) |
| Total central LNs,mean(SD)[range] | 11.13(8.25)[0–64] |
| Metastatic central LNs,mean(SD)[range] | 5.48(6.01)[0–37] |
| Total lateral LNs,mean(SD)[range] | 40.03(28.00)[5–161] |
| Metastatic lateral LNs,mean(SD)[range] | 8.67(7.34)[0–35] |
| Surgery | |
| total thyroidectomy | 63(52.9 %) |
| Lobectomy plus isthmusectomy | 56(47.1 %) |
| Follow-up duration, month(s) | 32.8(1–84) |
| Recurrence | 4(3.4 %) |
A total of 91(76.5 %) pediatric PTC patients visited for cervical masses. Twenty-eight (23.5 %) were asymptomatic and detected by physical examinations. No patient had shortness of breath or hoarseness. Total thyroidectomy was performed in 63 (52.9 %) patients, while 56 (47.1 %) underwent lobectomy plus isthmusectomy. All patients received central lymphadenectomy(CND), and 60 (50.4 %) underwent bilateral CND. 61 (51.3 %) patients underwent lateral lymphadenectomy (LND) and bilateral LND was performed in 19 patients.
The rates of CLNM and LLNM were 79.0 % (n = 94/119) and 49.6 % (n = 59/119), respectively. The mean (SD) number of lymph nodes resected per lateral neck (lymph node yield) was 40.03 (28), with a range of 5–161. The mean (SD) lymph node yield per central neck was 11.13 (8.25), ranging from 0 to 64. The mean number of positive central and lateral lymph nodes was 5.48 and 8.67, respectively. After a mean follow-up of 32.8 months, lymph node recurrence was found in 4 of 101 patients (3.4 %) with PTC.
DSV-PTC features
No patients younger than 11 years were diagnosed with DSV-PTC ( Table 2 ). Of the 18 DSV-PTC patients, 14 were females. There were no significant differences in age and sex at diagnosis between patients with DSV-PTC and those with C-PTC ( p > 0.05). Among the 18 DSV-PTC patients, 17 (94.4 %) had bilateral tumors, while only one had a unilateral tumor. Of the 101 patients with C-PTC, 44 had multifocal tumors, and 30 had bilateral tumors. Multifocality and bilateral tumors were significantly more common in DSV-PTC compared to C-PTC (100 % vs. 43.6 % and 94.4 % vs. 29.7 %, respectively; p < 0.001). All patients with DSV-PTC underwent LLND and CLND, with all 18 DSV-PTC patients having CLNM and LLNM. CLNM was found in 76 (75.2 %) C-PTC cases, and 42 (41.6 %) cases had LLNM. CLNM and LLNM were significantly more common in DSV-PTC compared to C-PTC ( p = 0.039 and < 0.001, respectively). There were a greater number of metastatic central LNs in DSV-PTC than in C-PTC ( p = 0.001).However, there were no significant differences in the presence of Hashimoto thyroiditis, ETE, lymphatic invasion, or the number of metastatic lateral lymph nodes resected between DSV-PTC and C-PTC. No patient in DSV-PTC group had recurrence, but four C-PTC patients (4.0 %) developed local recurrences. Lung metastasis occurred in 2 (11.1 %)DSV-PTC and 1(1.0 %) C-PTC patients at initial presentation, respectively.14(77.8 %) of DSV-PTC and 77(76.2 %) of C-PTC patients present with neck masses. But these differences were not significant ( p > 0.05). However, unlike C-PTC, DSV-PTC presents with diffuse involvement of one or both lobes of the thyroid gland without forming a dominant mass.
| Variables | DSV-PTC | C-PTC | P-value |
|---|---|---|---|
| Mean (SD) [Range]; (%) | Mean (SD) [Range]; (%) | ||
| Sex(female) | 14(77.8 %) | 75(74.3 %) | 0.982 |
| Age(<11 yrs) | 0(0 %) | 6(5.9 %) | 0.634 |
| Manifestations(neckmass) | 14(77.8 %) | 77(76.2 %) | 0.887 |
| ETE | 4(22.2 %) | 29(28.7 %) | 0.779 |
| HT | 10(55.6 %) | 36(35.6 %) | 0.110 |
| Lymphatic invasion | 3(16.7 %) | 8(7.9 %) | 0.460 |
| Multifocal | 18(100 %) | 44(43.6 %) | 0.000 * |
| Bilateral | 18(100 %) | 30(29.7 %) | 0.000 * |
| CLNM | 18(100 %) | 76(75.2 %) | 0.039 * |
| LLNM | 18(100 %) | 42(41.6 %) | 0.000 * |
| Central LNs | 17.17(3.21) | 12.70(0.86) | 0.008 * |
| Lateral LNs | 57.22(8.52) | 32.84(3.09) | 0.008 * |
| Metastatic central LNs | 10.28(2.03) | 7.37(0.85) | 0.001 * |
| Metastatic lateral LNs | 10.89(2.11) | 7.74(0.98) | 0.219 |
| Distant metastases | 2(11.1 %) | 1(1.0 %) | 0.059 |
Related posts:
 Surgical complications and functional outcomes of 3191 jejunal free flaps used for reconstruction of circumferential defects following head and neck cancer resections: A systematic review
Surgical complications and functional outcomes of 3191 jejunal free flaps used for reconstruction of circumferential defects following head and neck cancer resections: A systematic review
 Submandibular gland transfer into the temporal fossa in patients with oral squamous cell carcinoma: A viable option to prevent radiation-induced xerostomia
Submandibular gland transfer into the temporal fossa in patients with oral squamous cell carcinoma: A viable option to prevent radiation-induced xerostomia
 Predictors of recurrence and survival after salivary gland cancer surgery: A multicenter, retrospective study in northern Japan
Predictors of recurrence and survival after salivary gland cancer surgery: A multicenter, retrospective study in northern Japan
 The 10 %-rule debate: A fresh perspective on sentinel lymph node biopsy in OSCC
The 10 %-rule debate: A fresh perspective on sentinel lymph node biopsy in OSCC
 Deciphering molecular relapse and intra-tumor heterogeneity in non-metastatic resectable head and neck squamous cell carcinoma using circulating tumor DNA
Deciphering molecular relapse and intra-tumor heterogeneity in non-metastatic resectable head and neck squamous cell carcinoma using circulating tumor DNA
 Prophylactic gastrostomy tube during chemoradiation for head and neck cancer decreases weight loss but increases rate of tube use beyond six months
Prophylactic gastrostomy tube during chemoradiation for head and neck cancer decreases weight loss but increases rate of tube use beyond six months
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


