Anal canal cancer is rather an uncommon disease but its incidence is increasing. Squamous cell carcinoma (SCC) is the most frequent primary anal neoplasm and can encompass a variety of morphologies. HPV infection has a key role in precancerous lesions and cancer development by the production of E6 and E7 oncoproteins. Anal squamous precancerous lesions are now classified according to the same criteria and terminology as their cervical counterparts. The p16 expression by immunohistochemistry is a surrogate marker for human papilloma virus (HPV). Many other tumor types can arise in the anal canal, including adenocarcinomas, neuroendocrine tumors, malignant melanomas, lymphomas and various types of mesenchymal tumors. For differential diagnosis, immunostaining markers such as CK5/6 and p63 can be used to distinguish SCC and CK7 for adenocarcinoma. Other classical panels can also be applied as in other locations. Currently, there are no biomarkers able to predict prognosis or response to treatment in clinical practice.
Key points
- •
Anal cancer is an uncommon tumor, squamous cell carcinoma (SCC) being the most frequent histology corresponding to 80% of all cases.
- •
Human papilloma virus (HPV) infection plays a key role in anal cancer development, encoding at least three oncoproteins with stimulatory properties.
- •
SCC expresses CK5/6, CK 13/19, and p63. P16 is a surrogate marker for the presence of HPV genome in tumor cells.
Introduction
Anal cancer accounts for approximately 2.4% of gastrointestinal malignancies. Although anal cancer is a rare tumor, its frequency is increasing, especially in high-risk groups. Tumors in this location are generally classified as anal canal or anal margin.
Squamous cell carcinoma (SCC) is the predominant type of tumor and shares many features with cervical cancer. Oncogenic human papilloma virus (HPV) infection plays a major role in both tumors. HIV infection is associated with a higher frequency of HPV-associated premalignant lesions and invasive tumors.
Normal Anatomy of the Anus
The anal canal is the terminal part of the large intestine and is slightly longer in male than in female patients. It measures approximately 4 cm and extends from the rectal ampulla (pelvic floor level) to the anal verge, which is defined as the outer opening of the gastrointestinal tract. The anal verge is at the level of the squamous-mucocutaneous junction with the perianal skin.
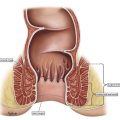
The dentate line (also called pectinate) consists of the anal valves and bases of the anal columns. It represents the anatomic division of the rectum from the anal canal. The dentate line originates from the embryonic union of the ectoderm with the endoderm. The anal canal epithelium can be divided into three zones ( Fig. 1 ). The upper part consists of colorectal mucosal type, followed by an anal transition zone (ATZ) that is composed of specialized epithelium that starts at the dentate line and extends from 0.5-1 cm. Finally, the distal anal canal consists of squamous epithelium, which may be partially keratinized. The anatomic distribution is clinically significant because it is related to lymphatic drainage and different types of precursor epithelium.
The tumor can be accessed for biopsy using anoscopy, rectoscopy, or direct examination of anal and perineal exophytic lesions.
Histology Classification
Tumors of the anal canal were classified by the World Health Organization (WHO) in three main groups: epithelial, mesenchymal, and secondary tumors. Epithelial tumors were subdivided into malignant and premalignant lesions ( Box 1 ).
- •
Epithelial tumors
- ○
Premalignant lesions
- ▪
Anal intraepithelial neoplasia (dysplasia), low-grade
- ▪
Anal intraepithelial neoplasia (dysplasia), high-grade
- ▪
Bowen disease
- ▪
Perianal squamous intraepithelial neoplasia
- ▪
Paget disease
- ▪
- ○
Carcinoma
- ▪
SCC
- ▪
Verrucous carcinoma
- ▪
Undifferentiated carcinoma
- ▪
Adenocarcinoma
- ▪
Mucinous adenocarcinoma
- ▪
- ○
Neuroendocrine neoplasms
- ▪
Neuroendocrine tumor (NET)
- •
NET G1 (carcinoid)
- •
NET G2
- •
- ▪
Neuroendocrine carcinoma (NEC)
- •
Small cell NEC
- •
Large cell NEC
- •
- ▪
Mixed adenoneuroendocrine carcinoma
- ▪
- ○
- •
Mesenchymal tumors
- •
Secondary tumors
Human Papilloma Virus Infection
Evidence indicates an association between oncogenic HPV infection with premalignant and malignant lesions of the genital tract, including the anus. The presence of HPV in anal cancer is variable and may be influenced by the methodology used for virus identification and by population characteristics. The HPV infection can be detected in tumor tissue using different techniques, including in situ hybridization ( Fig. 2 ) and polymerase chain reaction (PCR).
Currently, 88% of anal SCC tumor samples are usually HPV positive, with different rates according to geographic location. HPV16 infection is the most common, present in 86% of cases. In some cases, coinfection was found with multiple HPV types.
HPV is a nonenveloped virus with double-stranded DNA in circular form, containing a genome of around 8000 base pairs. HPV can remain housed in the nuclei of basal epithelial cells for decades after initial infection of the mucosa, which usually occurs through sexual contact. There are more than 240 types described and the alpha human papillomavirus is usually related to mucosal infection. The high-risk HPV genotypes (16 and 18) encode at least 3 oncoproteins with stimulatory properties: E5, E6, and E7. Integration of the viral DNA in the genome of the host cell is important for the progression of preneoplastic lesions to invasive carcinoma. During HPV integration, breakage of the E2 region of the viral genome occurs in the DNA of the infected cells, which causes the loss of suppressor function of the E2 protein. This results in an increased expression of the E6 and E7 proteins and their stimulation promotes invasiveness and keratinocyte immortalization. E6 and E7 expression is required for the induction and maintenance of the transformed state of HPV-related neoplasm. The protein E7 interacts with Rb protein (pRb) and E6 is able to bind and inactivate P53.
Introduction
Anal cancer accounts for approximately 2.4% of gastrointestinal malignancies. Although anal cancer is a rare tumor, its frequency is increasing, especially in high-risk groups. Tumors in this location are generally classified as anal canal or anal margin.
Squamous cell carcinoma (SCC) is the predominant type of tumor and shares many features with cervical cancer. Oncogenic human papilloma virus (HPV) infection plays a major role in both tumors. HIV infection is associated with a higher frequency of HPV-associated premalignant lesions and invasive tumors.
Normal Anatomy of the Anus
The anal canal is the terminal part of the large intestine and is slightly longer in male than in female patients. It measures approximately 4 cm and extends from the rectal ampulla (pelvic floor level) to the anal verge, which is defined as the outer opening of the gastrointestinal tract. The anal verge is at the level of the squamous-mucocutaneous junction with the perianal skin.
The dentate line (also called pectinate) consists of the anal valves and bases of the anal columns. It represents the anatomic division of the rectum from the anal canal. The dentate line originates from the embryonic union of the ectoderm with the endoderm. The anal canal epithelium can be divided into three zones ( Fig. 1 ). The upper part consists of colorectal mucosal type, followed by an anal transition zone (ATZ) that is composed of specialized epithelium that starts at the dentate line and extends from 0.5-1 cm. Finally, the distal anal canal consists of squamous epithelium, which may be partially keratinized. The anatomic distribution is clinically significant because it is related to lymphatic drainage and different types of precursor epithelium.
The tumor can be accessed for biopsy using anoscopy, rectoscopy, or direct examination of anal and perineal exophytic lesions.
Histology Classification
Tumors of the anal canal were classified by the World Health Organization (WHO) in three main groups: epithelial, mesenchymal, and secondary tumors. Epithelial tumors were subdivided into malignant and premalignant lesions ( Box 1 ).
- •
Epithelial tumors
- ○
Premalignant lesions
- ▪
Anal intraepithelial neoplasia (dysplasia), low-grade
- ▪
Anal intraepithelial neoplasia (dysplasia), high-grade
- ▪
Bowen disease
- ▪
Perianal squamous intraepithelial neoplasia
- ▪
Paget disease
- ▪
- ○
Carcinoma
- ▪
SCC
- ▪
Verrucous carcinoma
- ▪
Undifferentiated carcinoma
- ▪
Adenocarcinoma
- ▪
Mucinous adenocarcinoma
- ▪
- ○
Neuroendocrine neoplasms
- ▪
Neuroendocrine tumor (NET)
- •
NET G1 (carcinoid)
- •
NET G2
- •
- ▪
Neuroendocrine carcinoma (NEC)
- •
Small cell NEC
- •
Large cell NEC
- •
- ▪
Mixed adenoneuroendocrine carcinoma
- ▪
- ○
- •
Mesenchymal tumors
- •
Secondary tumors
Human Papilloma Virus Infection
Evidence indicates an association between oncogenic HPV infection with premalignant and malignant lesions of the genital tract, including the anus. The presence of HPV in anal cancer is variable and may be influenced by the methodology used for virus identification and by population characteristics. The HPV infection can be detected in tumor tissue using different techniques, including in situ hybridization ( Fig. 2 ) and polymerase chain reaction (PCR).
Currently, 88% of anal SCC tumor samples are usually HPV positive, with different rates according to geographic location. HPV16 infection is the most common, present in 86% of cases. In some cases, coinfection was found with multiple HPV types.
HPV is a nonenveloped virus with double-stranded DNA in circular form, containing a genome of around 8000 base pairs. HPV can remain housed in the nuclei of basal epithelial cells for decades after initial infection of the mucosa, which usually occurs through sexual contact. There are more than 240 types described and the alpha human papillomavirus is usually related to mucosal infection. The high-risk HPV genotypes (16 and 18) encode at least 3 oncoproteins with stimulatory properties: E5, E6, and E7. Integration of the viral DNA in the genome of the host cell is important for the progression of preneoplastic lesions to invasive carcinoma. During HPV integration, breakage of the E2 region of the viral genome occurs in the DNA of the infected cells, which causes the loss of suppressor function of the E2 protein. This results in an increased expression of the E6 and E7 proteins and their stimulation promotes invasiveness and keratinocyte immortalization. E6 and E7 expression is required for the induction and maintenance of the transformed state of HPV-related neoplasm. The protein E7 interacts with Rb protein (pRb) and E6 is able to bind and inactivate P53.
Preinvasive lesions
There are different terminologies used to describe premalignant lesions of the anal region. Squamous lesions were first described in the anal margin 50 years ago and they were initially classified as cutaneous lesions, such as Bowen disease and carcinoma in situ. Over time, a causal relationship was established between anal dysplasia and HPV perianal infection. However, terminologies of squamous precancerous lesions of anal canal continued to be diverse. The WHO classification ( Box 1 ), for instance, has four items related to premalignant squamous lesions. There are two items grading intraepithelial neoplasia/dysplasia in low and high grade. In addition, two other categories, Bowen disease, and perianal squamous intraepithelial neoplasia. These last two probably designating the same lesion. To make things even more complicated, the American Joint Committee on Cancer (AJCC) definition for primary tumors classifies noninvasive squamous lesions as carcinoma in situ, Bowen disease, high-grade squamous intraepithelial lesion (HSIL), and anal intraepithelial neoplasias (AIN) 2-3. This shows the need to propose a clearer classification so that the work of clinicians and pathologists is more uniform.
Squamous Intraepithelial Lesions
Because HPV plays a causal role in perianal and anal neoplasia, anal squamous precancerous lesions should now be classified according to the same criteria and terminology as their cervical counterparts using the Lower Anogenital Squamous Terminology (LAST) system.
A consensus process was organized by the College of American Pathologists and the American Society for Colposcopy and Cervical Pathology to recommend terminology unified across lower anogenital sites. The aim of this system of standardization was to create uniformity in histologic nomenclature for HPV-associated tumors that occurred in the anogenital tract. This permits a better use of current biomarkers and enables an efficient communication between specialties that establish the diagnosis and treatment of these lesions. The recommendation for classifying preinvasive lesions in the anal canal was similar to the cervical site. Hence, the same two-tiered nomenclature of intraepithelial lesion could be applied: low-grade squamous intraepithelial lesion (LSIL) and HSIL. The lesions are located above the basement membrane and may originate from the transitional or squamous epithelium of the anal canal. In the LAST system, condyloma is located with LSIL in the same category and Bowenoid papulosis is considered a special form of HSIL. Besides this, it does not discriminate cytologic from tissue specimens. Therefore, the terms LSIL and HSIL can be used in both materials. However, for histopathological diagnosis, the suffix AIN can be used; therefore, the lesion in the anal canal can be subcategorized as: LSIL-AIN 1 and HSIL-AIN 2–3.
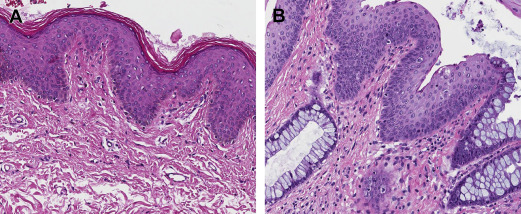
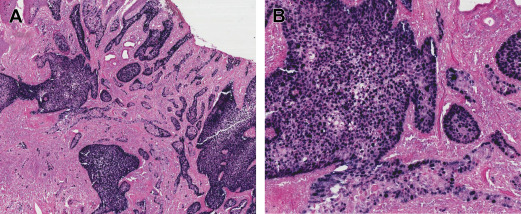
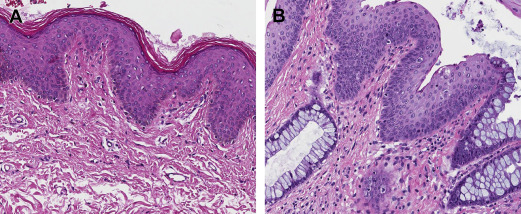
LSIL-AIN 1 can be defined as a proliferation of metaplastic squamous cells with nuclear atypia in the lower third of the epithelium or demonstrating koilocytotic changes in a papillary lesion ( Fig. 3 ). The histologic findings of HSIL-AIN 2-3 consist of a thickened proliferating epithelium containing atypical cells showing abnormal nuclear polarity, nuclear pleomorphism, and high nuclear hyperchromatism: cytoplasmic ratio and increased mitotic activity ( Fig. 4 ).
Related posts:
 Patient Perspective and Personal Journey of Treating a “Rare Cancer”
Evolution and Management of Treatment-Related Toxicity in Anal Cancer
Patient Perspective and Personal Journey of Treating a “Rare Cancer”
Evolution and Management of Treatment-Related Toxicity in Anal Cancer
 Human Immunodeficiency Virus/AIDS, Human Papillomavirus, and Anal Cancer
Human Immunodeficiency Virus/AIDS, Human Papillomavirus, and Anal Cancer
 Diagnosis and Diagnostic Imaging of Anal Canal Cancer
Treatment of the Primary Tumor in Anal Canal Cancers
Diagnosis and Diagnostic Imaging of Anal Canal Cancer
Treatment of the Primary Tumor in Anal Canal Cancers
 Locally Recurrent Disease Related to Anal Canal Cancers
Locally Recurrent Disease Related to Anal Canal Cancers
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


