CASE 44
FG, a 42-year-old patient with fulminant cardiac failure secondary to acute viral myocarditis, receives a heart (via UNOS) from a trauma victim. You are aware incidentally that the lungs, liver, and kidneys of the same donor have been used in other transplants around the globe.
QUESTIONS FOR GROUP DISCUSSION
RECOMMENDED APPROACH
Implications/Analysis of Family History
We are not provided with any family history for the patient.
Implications/Analysis of Clinical History
Acute and Chronic Rejection
Chronic rejection occurs with release of a variety of mediators, including fibroblast growth factor and endothelial growth factor, which can cause an insidious fibrosing/proliferative reaction relatively refractory to immunosuppressive treatment. This could affect the heart, causing secondary lung failure (and the respiratory distress). However, the kinetic picture (<4 weeks after transplant) does not suggest this as a likely explanation.
Implications/Analysis of Laboratory Investigation
Side Effects of Drug Therapy
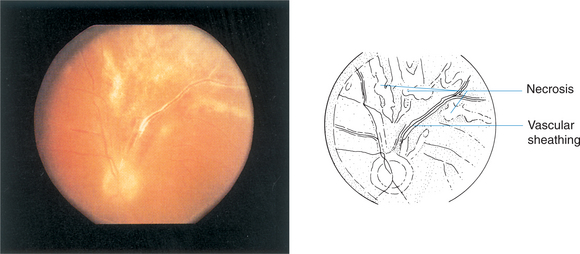
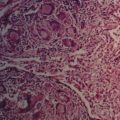
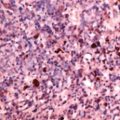
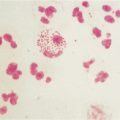
Could this disorder represent one of a possible number of side effects of the treatment he received for the transplant? In general, we know that chronically immunosuppressed populations show an increased frequency of malignancy, drug toxicity, and infections (Fig. 44-1).



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


