Case study 34.1
A 52-year-old Caucasian man is referred to you with abnormal blood counts. The white blood cell (WBC) count is 3000/μl, absolute neutrophil count (ANC) 1800/μl, hemoglobin 11 g/dl, and platelet count 130,000/μl. Further work-up reveals an enlarged spleen of 14.5 cm. The patient continues to work full-time as a bank manager. He denies B-symptoms or recurrent infections.
1. All of the following statements with regard to the diagnosis of hairy cell leukemia (HCL) are true EXCEPT:
- Bone marrow examination usually shows a hypercellular marrow with increased reticulin fibrosis, mast cells, and absence of blasts
- Monocytopenia is seen in almost all cases
- Flow cytometry is negative for CD25 and CD22
- There is absolutely no specific immunophenotypic marker for the diagnosis of HCL
- Immunohistochemistry (IHC) is positive for DBA.44, TRAP, and ANXA1
HCL is a rare B-cell lymphoproliferative neoplasm that represents approximately 2% of all leukemias and affects 600–800 individuals annually in the United States. HCL is more common in Caucasians than African Americans and is more common in males by a ratio of 4:1. The median age at disease onset is 52 years. HCL is characterized by clonal proliferation of small, mature lymphocytes with classic “hair-like” cytoplasmic projections that accumulate in the peripheral blood, bone marrow, and spleen (Figure 34.1). This leads to decreased production of normal hematopoietic elements, causing anemia, thrombocytopenia, and neutropenia and monocytopenia. Splenomegaly is usually present and may be massive; however, lymphadenopathy is rare except in relapsed disease. Patients typically present with either incidental or symptomatic cytopenias or abdominal symptoms from splenomegaly. Leukocytosis is unusual, and most patients (60–80%) are pancytopenic at diagnosis. On bone marrow examination, the marrow is typically hypercellular with diffusely infiltrating hairy cells, and abundant cytoplasm surrounding nuclei may give cells a “fried-egg” appearance. There is often increased reticulin fibrosis (due to hairy cell infiltration), and there may also be an increased number of bone marrow mast cells. Blasts are not increased. Immunophenotyping by flow cytometry is an important, confirmatory test for the diagnosis of HCL, which has a characteristic immunophenotypic profile consisting of both mature B cell markers (CD19, CD20, and CD22) and aberrant expression of non-B-cell markers (CD11c, CD25, CD103, and CD123). However, there is no one marker or combination of markers that is 100% specific for the disease. Immunohistochemical stains for DBA.44, TRAP, and ANXA1 are typically positive in HCL but have been largely replaced by flow cytometry.
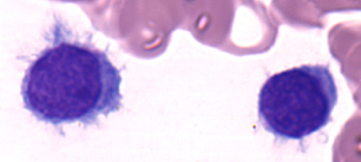 Figure 34.1 Hairy cells with classic circumferential, hairlike cytoplasmic projections. (Color plate 34.1)
Figure 34.1 Hairy cells with classic circumferential, hairlike cytoplasmic projections. (Color plate 34.1)
2. All of the following neoplasms are considered in the differential diagnosis of patients presenting with splenomegaly and B-cell lymphoid aggregates in the bone marrow EXCEPT:
- Splenic marginal zone lymphoma (SMZL)
- Prolymphocytic leukemia (PLL)
- Chronic lymphocytic leukemia (CLL)
- HCL variant (HCL-v)
- Primary myelofibrosis (PMF)
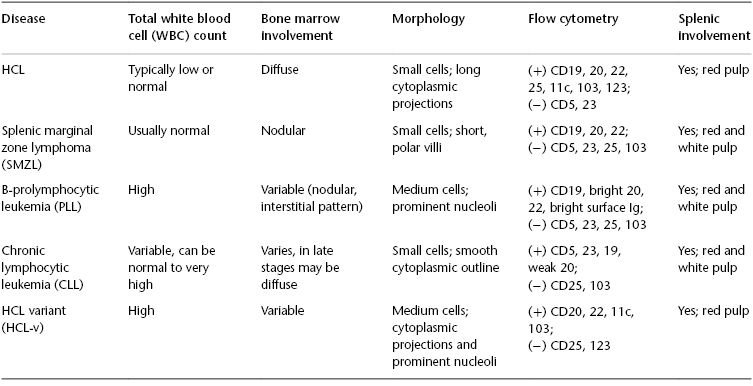
Primary myelofibrosis is a myeloid malignancy, and while it may cause splenomegaly it would not result in lymphoid aggregates in the bone marrow. See Table 34.1 for characteristics of A–D in relation to HCL.
Table 34.1 Characteristics of various neoplasms in relation to hairy cell leukemia (HCL).
3. The bone marrow biopsy of the patient presented in Question 1 shows a hypercellular marrow, but the marrow was inaspirable (a “dry tap”). Reticulin stain shows 2+ fibrosis surrounding hairy cells. Both flow cytometry on the peripheral blood and IHC on the marrow are consistent with the diagnosis of HCL. Should this patient be treated or observed?
This patient should be observed. Many patients with HCL are asymptomatic and can be observed for months to years before requiring treatment. HCL is typically idolent and slowly progressive, and there is no clear benefit to early treatment. Patients should be treated only when they become symptomatic or develop significant cytopenias. Typical indications for the treatment of HCL include an ANC <1000/μl, symptomatic anemia with hemoglobin <11 g/dl, and platelet count <100,000/μl. Symptomatic splenomegaly—early satiety, abdominal fullness and discomfort, and weight loss—is also an indication for treatment. Bulky lymphadenopathy at initial presentation is rare, and other diagnostic possibilities should be considered if present. Constitutional symptoms, such as fever and night sweats, should also prompt consideration of treatment after infection is ruled out. Infection should always be suspected and treated appropriately in a febrile patient with HCL; bacterial infections are most common, but opportunistic infections can occur as well.
 17: Management of Therapy-Related Myeloid Neoplasms
17: Management of Therapy-Related Myeloid Neoplasms
 36: Nodular Lymphocyte-Predominant Hodgkin Lymphoma
36: Nodular Lymphocyte-Predominant Hodgkin Lymphoma
 71: Secondary Brain and Spinal Cord Tumors
71: Secondary Brain and Spinal Cord Tumors



