2 Department of Paediatric Neurology, Evelina Children’s Hospital, Guy’s and St Thomas’ NHS Foundation Trust, London, UK
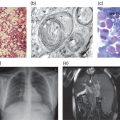
Batten disease or Neuronal Ceroid Lipofuscinosis (NCLs) is the collective name for a group of at least 11 fatal inherited storage disorders that share similar pathological and clinical features. The characteristic pathology common to all these disorders is the accumulation of autofluorescent storage material within the lysosome and the widespread death of neurons. Clinically these disorders typically involve visual failure, medically refractory epilepsy and relentless declines in motor and cognitive skills, invariably ending in premature death. Each NCL is caused by mutations in a different gene. Confusingly, these genes are called “CLN” genes, but more commonly the forms of NCL are referred to by the age of onset, e.g. infantile, late-infantile or juvenile NCL. A new classification scheme has been proposed (http://www.ucl.ac.uk/ncl/newnomenclature.shtml), which includes the name of the mutated gene (e.g. CLN1 disease, etc) and the age of onset seen in that individual. It is likely that all forms of nomenclature will remain in use, and this may vary between clinicians, affected families and the scientists investigating these disorders.
The most common NCLs in the UK are CLN1 disease, infantile (also known as infantile NCL, INCL); CLN2 disease, late-infantile (late-infantile NCL, LINCL) and CLN3 disease, juvenile (juvenile NCL, JNCL). In addition there are less common late-infantile variants (CLN5 disease, CLN6 disease, CLN7 disease and CLN8 disease), and the very rare congenital (CLN10 disease, CNCL) and adult-onset forms (ANCL).
Typical case scenarios
CLN2 disease, late infantile
A child is healthy and achieves developmental milestones as expected in the first year of life and there are no concerns. At 2 years she is walking independently but is not gaining fine motor skills as quickly as peers, and is not yet putting words together or able to point to body parts on demand. Just after her third birthday, the child has an unexplained sudden fall to the ground with rapid recovery. A few weeks later the child has a generalized convulsion lasting 3 minutes during an intercurrent febrile illness. The child goes on to have recurrent febrile and afebrile generalized motor seizures and is started on medication. However, the seizures are not easily controlled and within 12 months, she is on combination therapy for seizures, which include motor seizures, drop attacks and absences. Meanwhile developmental gains have slowed and the child has not learned any new words. At 5 years the child is becoming increasingly jerky and clumsy, is just able to sit without support, has lost all vocabulary and fine motor skills, and chewing and swallowing is becoming difficult. At this stage there are concerns that visual behaviour is deteriorating. The child is still visually responsive to large coloured objects and bright lights, and parents are clear that hearing and personality are retained. The seizures continue, but can be managed. Over the next few years, limb myoclonus with or without an EEG correlate, becomes more and more obvious. The jerks settle completely in sleep and are aggravated with moving and handling. By 6 years old, most children with CLN2 disease, late infantile, are completely dependent for all their everyday care needs, and vision is limited to light/dark differentiation. Feeding by nasogastric or gastrostomy tube is necessary. There is increasing pyramidal tract involvement with evolving limb spasticity and joint contractures. Head control is lost. Gut and chest problems increase and death occurs prematurely before or around adolescence.
The diagnosis is usually made when seizures become intractable and developmental standstill or regression is recognized, often a year or more after the onset of symptoms. CLN2 disease should be suspected if there is an occipital spike/wave response to slow photic stimulation on the EEG. It is confirmed by the finding of TPP1 deficiency in blood or fibroblasts and mutations on both alleles of the CLN2 gene.
CLN3 disease, juvenile
A child is healthy and achieves normal developmental milestones in the pre-school years. Between 4 and 7 years of age, vision deteriorates dramatically over a period of around 6–12 months. This is noticed as children struggle in the classroom, sit closer to the TV at home, start to not notice objects of interest or to look for things using hands in preference to vision. Low vision aids are useful for a while, but vision gradually declines further, reaching the level of light/dark awareness by the early teens. Children remain in good health for a number of years following the initial visual symptoms, but short-term memory and rate of learning may decline towards the end of primary school. The average age at the first seizure is around 10 years, but there may be long time intervals of many months or even years before subsequent seizures occur. During the early teenage years there is further slowing of thought and learning, and a slowly evolving Parkinsonian movement disorder, which affects speech as well as ambulation. There is a characteristic emotional/psychiatric phenotype but this is not seen universally. Many teenagers and young adults have episodes of acute anxiety, which may be associated with visual or sensory hallucinations. Restricted interests and topics of conversation are very common. Seizures gradually become more troublesome, requiring medical treatment, alongside deteriorating gait, speech and feeding skills. Understanding is preserved far longer than the ability to communicate easily with others and skilled care is needed. Personality and hearing are preserved until the end. Myoclonus, tremor and asymmetrical motor signs are seen occasionally. There is evidence to suggest that other systems are involved in the disease process, and some specialist centres advocate cardiac surveillance for rhythm abnormalities. Young adults become increasingly dependent for all their care needs, and death occurs at any time from early teenage to the fifth decade.
The diagnosis is now made most often soon after presentation with rapid sight impairment in the early school years. Sometimes children are given an initial diagnosis of a retinal dystrophy and CLN3 disease is not diagnosed until after the first seizure several years later. With a history of vision deteriorating over 6–12 months and an abnormal electroretinogram in a school-aged child there are few differential diagnoses. Blood can be sent for microscopic examination of a thick film to look for the presence of vacuolated lymphocytes. If these are present the diagnosis may be confirmed genetically. Over 80% of affected individuals are homozygous for a common 1-kb deletion of the CLN3 gene.
Only gold members can continue reading. Log In or Register to continue