12: Relapsed and Refractory Acute Myeloid Leukemia
Relapsed and Refractory Acute Myeloid Leukemia
Stefan H. Faderl
Hackensack University Medical Center, Hackensack, NJ, USA
Multiple Choice Questions
1. Which of the following factor(s) influence outcome at relapse?
Age at relapse
Duration of CR1
Cytogenetics at diagnosis
All of the above
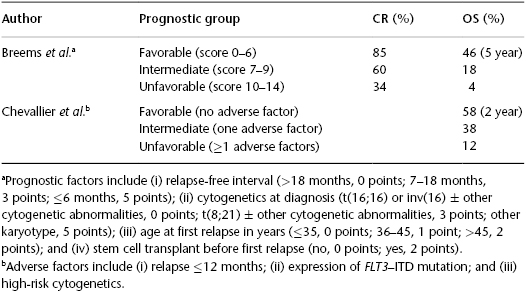
As has become clear, a substantial number of patients may not benefit from intensive re-induction chemotherapy and a search for investigational therapies (i.e., a clinical trial is more appropriate). Yet, on the other hand, a small group of patients may indeed benefit from attempts at intensive re-induction therapy and carry an altogether more favorable prognosis. Several prognostic indices have been devised to more accurately predict outcome for patients in first relapse. In a study by Breems et al. (2005) of 667 patients with AML in first relapse, four clinical parameters determined outcome: duration of CR1, cytogenetics at diagnosis, age at relapse, and whether or not previous HPCT was performed. Using a stratification system, three risk groups were identified with OS rates ranging from 46% at 5 years in the best prognosis group to 4% in the worst prognosis group (Table 12.2), which included the majority (almost 70%) of the patients. The GOELAMS group presented a simplified prognostic score based on a multivariate analysis of 138 patients with relapsed or refractory AML, which was then validated in an independent cohort of 111 patients. The three strongest independent adverse prognostic factors for OS included disease status (relapse within the first 12 months or later), FLT3–ITD-positive status, and high-risk cytogenetics. Accordingly, patients with no adverse factors had an OS of 58%, whereas patients in the highest risk group (two or more adverse factors) had an OS of 12% at 2 years. Applying these scores to the described patient, the 5-year OS is 4% and the 2-year OS is 12% in the study by Breems et al. (2005) and the GOELAMS group, respectively.
Table 12.2 Prognostic scoring systems in patients with AML in first relapse (Source: Adapted from Breems D, et al. J Clin Oncol. 2005;23:1969–78; and Chevallier P, et al. Leukemia. 2011;25:939–44).
2. True or false? Patients who relapse following high-dose cytarabine-based induction therapy are more likely to respond to salvage therapy than those who had received a standard dose cytarabine induction (e.g., “7 + 3”) therapy.
True
False
Although the 7 + 3 combination consisting of standard doses of cytarabine (100 to 200 mg/m2/dose) is the most widely used induction therapy, there is some evidence that higher doses of cytarabine during induction benefit younger adults (patients <60 years) and especially those patients <45 years of age. The question arises whether patients who fail to respond to higher-intensity induction regimens fare differently from those who relapse after a more standard and less intensive induction regimen. In a study of 1597 patients with AML between the ages of 18 and 85 years, 285 patients were refractory to HiDAC-based induction therapy. These patients on average tended to be older and were more likely to have a history of an antecedent hematologic disorder, blasts with unfavorable cytogenetics, and a higher WBC count at presentation. Only 43 patients (22%) responded to salvage therapy, and with a median follow-up of 72 months, only 11 patients stayed alive, mostly those who underwent an HPCT. The median survival of these patients was only 3.8 months, and among the patients who achieved remission, the median remission duration was only 9.1 months.
3. True or false? In adult AML, 1-year survival rates of up to 20% can still be achieved in some patients with multiple relapses.
 17: Management of Therapy-Related Myeloid Neoplasms
17: Management of Therapy-Related Myeloid Neoplasms
 11: Minimal Residual Disease in Acute Myeloid Leukemia
11: Minimal Residual Disease in Acute Myeloid Leukemia
 71: Secondary Brain and Spinal Cord Tumors
71: Secondary Brain and Spinal Cord Tumors



