Fig. 40.1
Coronal T1 MRI showing a giant pituitary multicystic macroadenoma
The sphenoid sinuses are variable in size and shape and are normally asymmetrical. Preoperative imaging gives the surgeon a map of the route to the gland. Image guidance can be very useful.
Endoscopic transsphenoidal route:
The nasal cavity is decongested in the anesthetic room once the patient is anesthetized.
The right middle turbinate is lateralized.
The natural sphenoid ostium in the sphenoethmoidal recess is identified, and the anterior wall of the sphenoid on both sides is removed inferiorly and medially widening the ostium. The arterial branches supplying the nasal septum run inferior to the natural sphenoid ostium and are preserved by pushing the mucosa inferiorly, prior to bone removal, in case a future nasoseptal flap is needed.
The posterior aspect of the septum is removed, approximately 1 cm anterior to the rostrum of the vomer, which is then also removed.
A long shafted bur may be useful if the bone here is thick.
Bone and mucosa are removed until a complete 360° view of anterior sella wall is achieved with at least an instrument width spare all around the pituitary fossa to allow space for instrument maneuverability during tumor removal (Fig. 40.2).
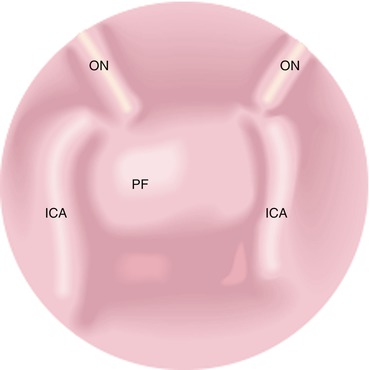
Fig. 40.2
Diagram of endoscopic view of the interior of the sphenoid sinus with the intersinus septum removed, showing the pituitary fossa (PF), optic nerves (ON), and internal carotid arteries (ICA)
The anterior bony wall of the pituitary fossa may be dehiscent, especially in macroadenomas, or occasionally (more commonly in microadenomas) be quite thick and needs drilling.
The dura mater lining the pituitary fossa needs to be incised to enter the gland with sharp dissection, diathermy, or laser. A thinner layer of pituitary capsule is deep to this, and the surgeon may try to develop a plane between the normal gland and the tumor capsule. If there is brisk cavernous bleeding, it is likely that the surgeon has not completely cut through the dura. There are usually interconnecting venous lakes (superior and inferior intercavernous sinuses) that may need to be controlled with pressure, hemostatic agents, diathermy, or Ligaclips.Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree





