Above-Knee Amputation
Daria Brooks Terrell
BACKGROUND
Although many bone and soft tissue sarcomas of the femur and thigh can be treated with limb-sparing techniques, some aggressive tumors are complicated by neurovascular involvement or extensive soft tissue contamination and thus require an above-knee amputation (AKA) (FIG 1).
An AKA is a transfemoral amputation of the lower extremity. AKAs are usually classified by level: high (just below the lesser trochanter), standard or midfemur (diaphyseal), or low distal femur (supracondylar).
In general, transfemoral amputations with 50% to 70% of the residual bone length (measured from the greater trochanter to the lateral femoral condyle) are optimal. However, when amputations are done in an oncologic setting, the amount of femur remaining is determined by the extent of the tumor.
Generally, if 3 to 5 cm of bone distal to the lesser trochanter remains, a standard AKA prosthesis can still be used.
ANATOMY
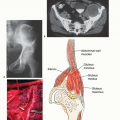
The surgeon must be familiar with the major neurovascular structures of the thigh because these structures will need to be identified and ligated. The femoral artery is the main artery of the thigh and femur. Its course changes throughout the length of the femur and, therefore, its location varies depending on the level of amputation (FIG 2).
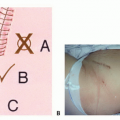
 FIG 1 • Primary bone sarcoma of the distal femur with a soft tissue (extraosseous) component can be treated with limb-sparing surgery and endoprosthetic reconstruction (A) or amputation (B). C. AKA for an osteosarcoma of the distal femur, performed in the early 1960s. Because of the lack of accurate imaging modalities at that time, the extent of the soft tissue component and the relation of the tumor to the neurovascular bundle were assessed in surgery using a large incision and only then was the decision to proceed with an amputation made. |
High Above-Knee Amputation
Proximally, the femoral artery lies beneath the sartorius muscle, anterior to the adductor longus muscle, and anterior to the femur. The profunda femoris artery lies posterior to the adductor longus muscle. At this level, the femoral artery is lateral to the femoral vein. The sciatic nerve lies posterior to the adductor magnus and anterior to the long head of the biceps.
Midfemur Above-Knee Amputation
The femoral artery lies between the vastus medialis and the adductor magnus and is medial to the femur in the midthigh area. In this region, the femoral vein is lateral to the artery. The sciatic nerve lies between the short head of the biceps and the semimembranosus.
 FIG 2 • Level of osteotomy and cross-sectional anatomy for supracondylar, diaphyseal, and high AKA. (Courtesy of Martin M. Malawer.) |
Supracondylar Above-Knee Amputation
The femoral artery is directly posterior to the femur. After passing the canal of Hunter, the femoral artery joins the sciatic nerve in the popliteal fossa. The artery is deep and medial to the sciatic nerve.
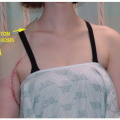
 FIG 3 • A. A 45-year-old patient initially presented with a dedifferentiated, highgrade osteosarcoma of the fibula. After neoadjuvant chemotherapy, the patient underwent intercalary fibular resection. Approximately a year after the surgery, the patient presented with a rapidly enlarging, extensive tumor recurrence. B. As shown on MRI, the tumor extensively invaded the superficial posterior, deep posterior, and lateral compartments of the leg. Wide excision of the tumor would necessitate removal of the neurovascular bundle and all three compartments. AKA was therefore performed. |
INDICATIONS
Local recurrence of malignant carcinoma or sarcoma where limb salvage would not yield a functional limb or effectively remove the disease (FIG 3A)
Tumors with major vascular involvement with invasion of major blood vessels, which usually have poor outcomes and a poor prognosis (FIG 3B)
Soft tissue contamination, such as after a pathologic fracture
Tumors of the distal lower extremity with major nerve involvement, as with tumors of the popliteal space (FIG 4A,B)
A poorly planned and executed biopsy, which can cause extensive contamination
Infection, particularly in the case of tumor ulceration
Skeletal immaturity, which often leads to significant limb length discrepancies when limb-sparing procedures are done on skeletally immature patients
Extensive tumor involvement that prohibits adequate soft tissue coverage of a prosthesis (FIG 4C-E)
IMAGING AND OTHER STAGING STUDIES
Plain Radiography
Plain radiographs often provide the first indication for the need for amputation and an initial estimate of the necessary amputation level.
Orthogonal views of the femur, tibia, and fibula can be helpful in showing tumor involvement and the extent of bony destruction, although, generally, up to 30% of the bony architecture has to be destroyed before radiographic findings are apparent (FIG 5A).
 FIG 4 • A,B. A 77-year-old patient presented with a high-grade soft tissue sarcoma that invaded the popliteal space and destroyed the proximal and midshaft areas of the tibia and fibula, resulting in the loss of peroneal function. C. A 23-year-old patient with a few years’ history of a neglected benign giant cell tumor of the distal femur with an extensive soft tissue component. D. A plain radiograph of the distal femur showing extensive bone destruction. The knee joint is in flexion contracture due to intractable pain. E. CT shows that only a thin rim of muscles is left. Adequate soft tissue coverage of a prosthesis was therefore not feasible and AKA was performed. (C-E: Courtesy of Martin M. Malawer.) |
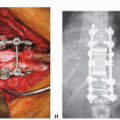
 FIG 5 • A. Plain radiograph of the knee showing extensive destruction of the proximal tibia and fibula. B. CT scan showing a large tumor that displaced the popliteal artery posteriorly and obliterated branches of the popliteal artery more distally. |
Computed Tomography and Magnetic Resonance Imaging
Computed tomography (CT) and magnetic resonance imaging (MRI) are the most helpful in determining the level of intramedullary tumor involvement and the extraosseous extent of the tumor, which is used to determine the amputation level (FIG 5B).Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree