Hematopoietic Stem Cell Transplantation for Nonmalignant Disorders
Hematopoietic Stem Cell Transplantation for Nonmalignant Disorders
Jacob R. Garcia
Mark C. Walters
INTRODUCTION
Hematopoietic stem cell transplantation (HSCT) has expanded significantly over the past several decades as a consequence of broader utilization in the treatment of malignant and premalignant conditions such as acute leukemia and myelodysplastic syndrome, respectively.1, 2 A parallel wider application also has evolved for nonmalignant disorders, such as hemoglobinopathies, primary immunodeficiency disorders (PIDs), inborn errors of metabolism, marrow failure syndromes, and other acquired and hereditary hematologic disorders, particularly among pediatric recipients.3, 4, 5, 6 Although supportive care for many of these conditions also has improved over this same period of time, long-term toxicity and morbidity of nontransplant interventions (e.g., chronic blood transfusions and iron overload) have a negative impact on the quality of life and can also cause early mortality.7 Thus, HSCT for nonmalignant disorders represents an alternative curative option for many patients who might otherwise succumb to complications of the underlying condition. In this chapter, we delineate and describe representative hereditary hematologic diseases for which HSCT is an option, review outcomes after HSCT in patients with these disorders, and outline the long-term effects of the therapy.
CONDITIONS SUITABLE FOR HEMATOPOIETIC STEM CELL TRANSPLANTATION
A broad array of hereditary and acquired nonmalignant disorders derives from selected hematopoietic cell lineages, which by virtue of their origin in the hematopoietic stem cell, also are theoretically amenable to cure by successful HSCT. Rather than attempt to catalog all these disorders, three broad categories of disorders have been selected to illustrate how and when to apply this therapeutic intervention.
The first of these are the PIDs, which classically are illustrated by the child with severe combined immunodeficiency syndrome (SCIDS) where there is absent B- and T-lymphocyte function. In these individuals, life-threatening infections occur in the first months of life and portend early mortality.8 Because there is no immunologic barrier to donor engraftment, marrow from an HLA-identical sibling can be infused in the absence of any pre-transplant immunosuppressive therapy. Thus, these were among the first cases in which the proof-of-principle of HSCT was demonstrated.
The next group of disorders are the hereditary bone marrow failure syndromes, of which Fanconi anemia (FA) is a prototypic example. Fanconi anemia is caused by a heterogeneous collection of defects in genes that encode proteins involved in DNA repair.9 This deficiency is associated with a variable phenotype that includes progressive aplastic anemia, musculoskeletal and other congenital defects, and cancer predisposition (particularly to myelodysplastic syndrome, acute myelogenous leukemia, and carcinoma of the skin and oropharynx).10 Although the hematologic manifestations of this condition are eliminated after successful HSCT, donor selection, modulation of the conditioning regimen, and the possibility of malignant transformation in the marrow together make this a challenging disease to treat by HSCT.
Finally, the broad category of hemoglobin disorders is discussed.11 These disorders differ from the others because the immune and hematopoietic systems are intact before HSCT, and a proliferative marrow develops as a consequence of chronic anemia and ineffective erythropoiesis. Thus, the conditioning regimen before HSCT for the hemoglobin disorders typically requires a combination of ablative and immunosuppressive activities. In addition, there is a marked variability of clinical phenotype in sickle cell disease, which affects the decision making about when and in whom to consider this aggressive therapy.
Together, these broad examples of nonmalignant conditions illustrate the variety of clinical and genetic parameters one must consider in selecting appropriate transplantation candidates and regimens. These considerations are highlighted in the sections that follow.
HEMATOPOIETIC STEM CELL TRANSPLANTATION FOR PRIMARY IMMUNODEFICIENCY DISORDERS
PIDs classically are associated with significant morbidity and early mortality caused by life-threatening infections in the first months and years of life. Before the availability of HSCT, these infections invariably caused death in the vast majority of affected children. SCIDS is the most widely recognized manifestation of a PID. SCIDS is a genetically heterogeneous group of over 20 mutations in 13 genes identified to date that result in the common phenotype of impaired T-cell production and/or function (Table 103.1). These mutations in varied target genes lead to impaired immunity as a consequence of absent T-cell function, but often defects in B-cell and natural killer (NK) cell number or function occur in parallel, as many of the genes affect all three lineages. However, the level of B- and NK-cell activity is highly variable. In rare cases, autoimmune phenomena are observed in these patients.13 This is particularly noteworthy in children with Omenn syndrome, which is caused by mutations in genes that participate in rearrangements of T-cell receptors and VDJ regions of immunoglobulins. Mutations in these genes elicit a phenotype that mimics graft-versus-host-disease as a consequence of the expansion of T-cell clones that are reactive to self-antigens. There is also reduced peripheral and central tolerance in these patients, which contributes to the observed phenotype.
Preparative Regimen
The first transplant for SCIDS using an HLA-matched sibling bone marrow donor was performed in 1968.14 In this case, no preparative regimen was administered to prevent graft rejection due to the absence of an immunologic barrier to engraftment. Thus, donor hematopoietic stem cells simply were infused and successful immune reconstitution followed. However, fatal graftversus-host disease (GVHD) often occurred in donor/recipient settings in which there was a major HLA disparity. By testing transplantation in animal models of SCIDS, it was determined that by using the technique of donor T-cell depletion, it was possible to eliminate GVHD after HLA-mismatched HSCT, if thorough T-cell depletion was accomplished.15, 16 In addition, after successful HSCT in the mouse, there was durable engraftment of the donor cells with restored host immunity. However, even in the earliest clinical reports of HSCT after T-cell depleted HLA-haploidentical HSCT for SCIDS, B-cell engraftment was quite poor, as most patients required long-term immunoglobulin replacement after HSCT.
TABLE 103.1 MOLECULAR CAUSES OF SEVERE COMBINED IMMUNODEFICIENCY
Common γ-chain (γc) of receptors for IL-2, -4, -7, -9, -15, and -21
45-50 (only males)
−
+
−
ADA
Adenosine deaminase enzyme
16
−
+
−
IL7R
α-Chain of IL-7 receptor
9
−
+
+
JAK3
Janus kinase 3, activated by γc
6
−
+
−
RAG1, RAG2
Recombinase activating genes required for T- and B-cell antigen receptor gene rearrangement
5
−
−
+
DCLRE1C (Artemis)
Part of T- and B-cell antigen receptor gene rearrangement complex, also required for DNA repair
<5
−
−
+
TCRD, TCRE, TCRZ
CD3 δ, ε, and ζ chains of the T-cell receptor complex, required for T-cell development
Rare
-/low
+
+
CD45
Protein tyrosine phosphatase receptor (PTPRC), required for T-and B-cell activation by antigen
Rare
-/low
+
+/low
LCK
Lymphocyte tyrosine kinase p56lck, required for T-cell development and activation
Rare
-/low
+
+
PNP
Purine nucleoside phosphorylase enzyme; deficiency also causes neurologic impairment
Rare
Low
Low
+/low
LIG4
DNA ligase IV required for antigen receptor gene rejoining
Rare
–
+
+
DNAPKCS
DNA protein kinase catalytic subunit, required for T- and B-cell antigen receptor rearrangement, and DNA repair
Rare
–
–
+
NHEJ1 (Cernunnos)
Nonhomologous end joining of DNA; deficiency also causes microcephaly and radiation sensitivity
Rare
–
–
+
AK2
Adenylate kinase 2; deficiency causes reticular dysgenesis with granulocytopenia, lymphocytopenia, and deafness
Rare
–
–
–
FOXN1
Forkhead box N1, required for thymus and hair follicle development (ortholog of nude mouse)
Rare
-/low
+
+
STAT5a
Signal transducer and activator of transcription 5, phosphorylated after cytokine receptor engagement; deficiency also causes growth-hormone-resistant growth failure
Rare
-/low
+
–
CORO1A
Coronin-1A, protein mediating lymphocyte migration and T-cell emigration from the thymus
Rare
-/low
+
+
Currently unknown
Unknown defects, including SCID and congenital anomalies; SCID with multiple bowel atresias
˜10
-/low
+/-
+/-
aBased on Buckley,18 Puck25 and Lindegren et al.12
bSome patients have substantial numbers of maternally derived T-cells at time of diagnosis; autologous T-cells are shown. Adapted from Puck JM. The case for newborn screening for severe combined immunodeficiency and related disorders. Ann N Y Acad Sci 2011;1246:108-117.
Epub 2012 Jan 13.
In a cohort of 161 patients treated by HSCT at a single U.S. institution, Railey et al. reported the results in individuals with SCIDS who received no pre-transplant chemotherapy or GVHD prophylaxis.17 Notably, only 16 (10%) of these patients had HLA-identical sibling donors, and thus most received T-cell depleted HLA-haploidentical marrow. In this clinical series, it was observed that survival was highest among those patients who were transplanted before 3.5 months of age (94% compared to 70%, P = 0.002). Of those who died, the majority (76%) experienced progressive viral infections that pre-dated HSCT. There were very few deaths related to GVHD or infections that were acquired after HSCT. Thus, this series suggested that no chemotherapeutic preparation is necessary in patients with SCIDS who are treated by HSCT shortly after birth. However, many patients require regular immunoglobulin (IVIG) infusions after successful HSCT for SCIDS due to absent engraftment of donor B-cells, particularly in the absence of a conditioning regimen before HLA-haploidentical related donor HSCT in recipients with B-cell positive SCIDS.18, 19
Long-term follow-up of patients showed mixed results regarding the stability of long-term donor T-cell engraftment after HLA-haploidentical HSCT in the absence of a conditioning regimen before HSCT. With up to 25 years follow-up in a report by Buckley, 11 of 19 patients had no evidence of decreased T-cell function or diminished T-cell repertoire diversity. However, as noted above, most patients lacked donor B-cell engraftment and thus received long-term replacement immunoglobulin therapy.8 In another series that included survivors with up to 16 years follow-up, 35% of the patients had low T-cell antigen receptor excision circle (TREC) levels and a limited T-cell repertoire as evidenced by oligoclonality that was demonstrated in 27.5% of patients.20 Based upon these observations, it has been suggested that the use of an ablative conditioning regimen before HSCT may be required to ensure long-term T-cell engraftment in the setting of HLA-haploidentical donors.
Whether improved T-cell engraftment translates into improved survival remains in question, however. Patel et al. retrospectively reviewed a series of 22 patients with SCIDS who were treated by HSCT at a single institution.21 In this series, no statistical difference in overall survival was with respect to whether a preparative regimen was administered regardless of donor type. In addition, experience from a large European cohort treated between 1968 and 2005 showed that chemotherapeutic preparation did not improve overall survival in patients with SCIDS.22 These authors argued that a conventional ablative chemotherapeutic preparation does not improve survival in patients with SCIDS, particularly in those who undergo HSCT in the first 31/2 months of life. Unfortunately, proceeding directly to HSCT early in life is not always feasible, as affected individuals often are not identified in the first several months of life or before they have developed serious infections. Thus, the decision of whether to use a conditioning regimen should hinge on several salient clinical features, including the patient’s age, the donor, and the baseline immunologic function with regard to resistance to donor engraftment. Also, recipients with SCIDS who have a T-/B+ lymphocyte profile appear to have better outcomes than recipients who lack B-cells.23 The advent of pilot newborn screening programs by TREC screening from blood spots has the potential to mitigate the limitation of patient age.24, 25, 26
Reduced Intensity Conditioning
To date, optimization of a conditioning regimen that might be safely applied in all patients with SCIDS has been elusive. In an attempt to reduce transplant-related morbidity and mortality, reduced intensity conditioning regimens that are not ablative and contain a diverse array of immunosuppressive agents such as fludarabine, busulfan (BU), etoposide, cyclophosphamide (CY), and low-dose radiation have been tested.27, 28, 29 Current data suggest that reduced intensity regimens are most appropriate in recipients with T-cell deficiency syndromes and in unrelated donor HSCT.30, 31 However, graft rejection associated with inadequate suppression of residual host immune function remains a concern, particularly in patients with T- and NK-cell function at baseline. Ultimately, the selection of a preparative regimen and its intensity will vary according to the level of retained immunity in the recipient, and with the degree of HLA matching in donor hematopoietic cells.
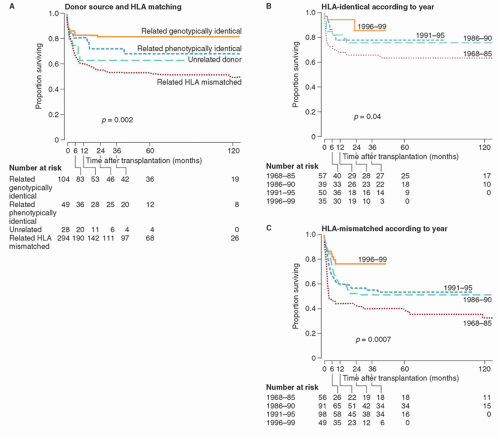
Donor Source
HLA-identical marrow HSCT has yielded very good results in SCIDS, with approximately 70% to 80% of patients surviving long-term32 (Fig. 103.1). Because most patients lack a HLA-ID sibling donor, alternative donor sources have been explored in clinical trials. Roifman et al. reviewed transplant outcomes after HLA-mismatched related donor HSCT compared to HLA-matched unrelated donor HSCT for SCIDS.33 They reported that survival was superior in those receiving HLA-matched unrelated marrow. Specifically, patients who received a HLA-matched unrelated HSCT had better engraftment and immune reconstitution. They concluded that HLA-matched unrelated marrow transplantation is superior to HLA-mismatched related donor HSCT and should be considered as the first choice when a related HLA-identical donor is unavailable. In other patient series noted above, excellent results were observed after T-cell depleted HLA-haploidentical HSCT. Thus, the optimal donor source for HSCT remains a point of controversy.
More recently, the application of umbilical cord blood transplantation (UCBT) has been explored in SCIDS. Fernandes et al. recently compared results after HLA-mismatched related donor and unrelated donor UCBT in patients with SCIDS.34 There were 175 HLA-mismatched donor HSCT recipients and 74 UCBT recipients in this retrospective cohort of patients with SCIDS or Omenn syndrome. The median follow-up was 58 and 83 months in each group, respectively. Most UCBT recipients received a myeloablative preparative regimen, whereas a larger fraction of the related donor recipients did not. UCBT recipients were more likely to have complete donor chimerism and faster lymphocyte recovery independent of the preparative regimen. T-cell engraftment was equivalent in the two groups, and immunoglobulin replacement was discontinued earlier after transplantation in the UCBT group. There was a statistically insignificant higher incidence of grade II—IV acute GVHD and statistically significant rate of chronic GVHD after UCBT. However, the 5-year overall survival rates were equivalent. Other data suggest that B-cell engraftment may be better after UCBT.35 Although a randomized, prospective trial has not been performed, these data indicate that UCB appears to represent a suitable alternative donor source.
Late Effects and Future Directions
There are limited series of long-term follow-up after HSCT for SCIDS in which the follow-up period exceeds 10 years.20, 21, 36 In several of these series, loss of T-cell diversity and autoimmune disorders was observed late after HSCT, although follow-up through 25 years after HSCT suggests improvement in the T-cell repertoire.37 In addition, patients with adenosine deaminase deficiency in particular have experienced a high incidence of central nervous system abnormalities that include motor dysfunction, sensorineural hearing loss, and cognitive deficits that contribute to emotional and behavioral difficulties.20 In addition, chronic infection by human papilloma virus also has been reported.20 It is unclear which, if any of these, is related to pre-transplant conditioning and GVHD prophylaxis or to the underlying genetic defect. Finally, for those who lack a transplant donor, gene therapy is an alternative therapy for some patients, although development of this technology is ongoing.38 A consensus group has discussed plans for future multicenter studies in North America, both retrospective and prospective, focused on collecting data from newborn screening and natural history sources.39 The importance of collaboration in developing new protocols for these rare disorders was illustrated best by recent data showing that long-term mortality rates for both SCIDS and non-SCIDS patients with a PID are higher than their age- and gender-matched controls in the general population.40
FIGURE 103.1. Overall survival after hematopoietic stem cell transplantation (HSCT) for severe combined immunodeficiency syndrome (SCIDS), according to donor stem cell source, degree of HLA matching, and the year of HSCT. Adapted from Antoine C, Muller S, Cant A, et al. Long-term survival and transplantation of haemopoietic stem cells for immunodeficiencies: report of the European experience 1968-99. Lancet 2003;361(9357):553-560. Epub 2003 Feb 25.
HEMATOPOIETIC STEM CELL TRANSPLANTATION FOR FANCONI ANEMIA
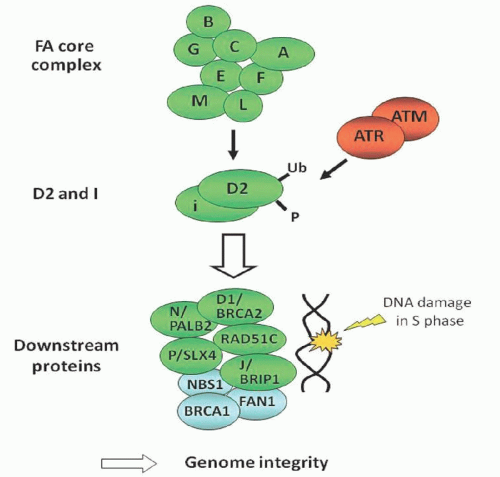
Fanconi anemia is the most common hereditary cause of bone marrow failure. The genetic defect responsible for these findings has been characterized in 15 complementation groups, termed FANC genes, most of which are autosomal and recessive (Table 103.2).41, 42 The most common mutations occur in FANCA, FANCC, FANCG, and FANCD2 genes. These gene products participate in a signal transduction pathway involved in DNA repair, called the FA/BRCA pathway (Fig. 103.2).43 Thus, its diagnosis is confirmed by a chromosome fragility test that when positive, should be followed by an attempt to define the complementation group by DNA testing.
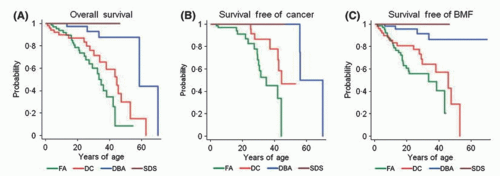
The most common hematologic manifestation is progressive marrow aplasia that causes cytopenias in the blood, which typically occur in the first or second decade of life.44 Erythrocyte macrocytosis and elevated fetal hemoglobin often are present. In some cases, the diagnosis of FA will not be established until after the patient has developed myelodysplastic syndrome or AML. Some patients never develop pancytopenia but do experience an increased risk of malignancy. Based upon studies of a cohort of FA patients at the NCI, the risks of developing MDS and AML by age 50 are estimated to be 40% and 10%, respectively.45, 46 The overall survival and cancer-free survival in this cohort is shown in Figure 103.3 with a median overall survival of 33 years in those with FA.
Because of poor survival, HSCT was developed as a therapeutic measure to restore normal hematopoiesis and reduce or eliminate the risk of hematologic malignancy. There were several important observations generated in the early clinical trials. The first was that high-dose alkylating chemotherapeutic drugs at doses administered for severe aplastic anemia and gamma irradiation caused severe toxicity including mucositis and hemorrhagic cystitis as a consequence of the sensitivity to DNA damage in all tissues.47, 48 Second, the risk of acute GVHD was increased in comparison to other indications for HSCT, presumably also as a consequence of impaired DNA repair and an extended duration of tissue injury eliciting an allogeneic reaction by donor T-cells.49 The initial reports by Gluckman and her colleagues in 1984 showed that a reduced-dose regimen of CY (20 to 40 mg/kg) and a single fraction of total body irradiation or thoracoabdominal irradiation (400 to 450 cGy) effectively modulated the toxicity and was sufficient to ensure engraftment after HLA-ID sibling bone marrow transplantation with a long-term survival rate of 58.5%, although the rates of acute (55%) and chronic (70%) GVHD were quite elevated.50 However, an updated experience of this regimen in 35 patients was reported in 2007, and included antithymocyte globulin (ATG) in the conditioning regimen.51 These results showed a probability of survival of 89% at 10 years, with the incidence of acute and chronic GVHD at 23% and 12%, respectively.
TABLE 103.2 GENES ASSOCIATED WITH FANCONI ANEMIA
Disease/Genes
Chromosome Locus
Mode of Inheritance Frequency
% of Patients
FANCA
16q24.3
AR
60
FANCB
Xp22.31
XLR
2
FANCC
9q22.3
AR
14
FANCD1/BRCA2
13q12.3
AR
3
FANCD2
3p25.3
AR
3
FANCE
6p21.3
AR
3
FANCF
11p15
AR
2
FANCG/XRCC9
9p13
AR
10
FANCI
15q25-26
AR
1
FANCJ/BACH1/BRIP1
17q22.3
AR
2
FANCL
2p16.1
AR
0.2
FANCM
14q21.3
AR
0.2
FANCN/PALB2
16p12.1
AR
0.7
FANCO
17q22
AR
I Case
FANCP
16p13.3
AR
I Case
FIGURE 103.2. FA/BRCA pathway. From Soulier J. Fanconi anemia. Hematol Am Soc Hematol Educ Program 2011;2011:492-497. Epub 2011 Dec 14.
FIGURE 103.3. Survival, cancer-free survival, and survival free of marrow failure in a cohort of patients with bone marrow failure syndromes from the National Cancer Institute. The probabilities of overall survival (A), survival free of cancer (B) and survival free of bone marrow failure (C) are depicted in the 3 panels among patients with Fanconi Anemia, Dyskeratosis Congenita, Diamond-Blackfan Anemia, and Schwachman-Diamond Syndrome. From Alter BP, Giri N, Savage SA, et al. Malignancies and survival patterns in the National Cancer Institute inherited bone marrow failure syndromes cohort study. Br J Haematol 2010;150(2):179-188. Epub 2010 May 29.
Several other notable improvements have occurred in the 25 years since these initial results after HSCT for Fanconi anemia were reported. The elimination of irradiation from the conditioning regimen has been associated with better results. In a series from Saudi Arabia, the replacement of thoracoabdominal irradiation by a combination of CY with ATG generated better results after HLA-ID sibling bone marrow transplantation (overall survival 96.9% versus 72.5%, P = 0.013).52 Alternatively, the use of CY alone at a reduced dose of 60 mg/kg by investigators in Brazil generated an overall survival and event-free survival 93% and 88%, respectively, with acute and chronic GVHD occurring in 71% and 28.5% of recipients after HLA-ID sibling transplantation.53 Thus, in patients who have a HLA-ID sibling donor and who have not yet progressed to MDS or AML, the results of the reduced intensity conditioning regimens are excellent. In addition, by eliminating radiation from the conditioning regimen, the risk of developing a malignancy after transplantation also should be lowered.
Only gold members can continue reading. Log In or Register to continue